A retrocerebellar cyst is often a congenital formation in the brain structures of the cerebellar-stem localization. The pathology is manifested by stem (nausea, vomiting, dizziness and weakness, tinnitus, increased sweating and hyperemia of the skin) and cerebellar symptoms (ataxia - impaired motor coordination).
Characteristics of the pathology
A retrocerebellar cyst is a cavity in the brain that has dense walls and often liquid contents, which makes it look like a capsule. A retrocerebral cyst is a cavity formed in the brain tissue, mostly congenital. The walls are formed from cells of the arachnoid membrane or fragments of gray matter.
The contents are often a liquid fraction, sometimes with fragments of soft tissue. The prevalence of the pathology is about 1-4% of all space-occupying formations localized in the brain. Retrocerebellar location means that the cyst is located behind the cerebellum.
Often the formation is localized in the area of the cerebral-cerebellar cistern - a large natural cavity filled with cerebrospinal fluid. The cistern is limited by the medulla oblongata and the cerebellum. A retrocerebellar arachnoid cyst formed in the brain becomes dangerous when its size increases significantly, causing compression of the surrounding brain structures.
Symptoms
What sizes are dangerous: a cyst manifests itself clinically when its size exceeds 3 cm in diameter. Retrocerebellar cyst of the brain is characterized by the following syndromes:
- Syndrome of increased intracranial pressure. Signs: bursting headache, dizziness, loss of appetite, sleep disturbance, irritability, emotional lability, decreased visual accuracy, tinnitus. Psychomotor development may be delayed in children.
- General cerebral symptoms: throbbing headache, drowsiness, stupor, memory loss, increased distractibility, seizures, tremors of the limbs. Patients answer questions slowly and are disoriented.
- Neurological deficit: decreased sensitivity, weakened muscle strength in the arms and legs.
- Focal symptoms. It is caused by mechanical compression of the cerebellum by the cyst. In this case, a retrocerebellar cyst of the cerebellum is manifested by impaired coordination, decreased accuracy of movements and gait disorder.
Classification
In the ICD-10 list, a retrocerebellar cyst is listed under the code “Q04.6”. In the ICD-10 list, an arachnoid cyst formed in the brain is also listed under the code “Q04.6”; this section is devoted to congenital cystic formations localized in the brain. Depending on the dynamics of development, progressive (gradually increasing in diameter) and stable (maintaining original dimensions) are distinguished. Taking into account the peculiarities of the formation of a cystic cavity, the following types are distinguished:
- True (isolated, represented by a dense shell with contents).
- Diverticular (communicating, formed in the late stages of embryogenesis as a result of disruption of the process of liquor dynamics).
- Valvular (partially communicating with natural liquor ducts and cavities, formed due to changes in the morphological structure of the arachnoid membrane).
Arachnoid cysts located in the brain are divided into small, medium and large, taking into account their size - the presence of cystic formations that do not entail undesirable consequences, in particular, the appearance of neurological symptoms, can be considered a normal variant.
Cystic formations of large diameter are often associated with restriction and deformation of reserve intracranial spaces. In severe cases, mass effect (compression of brain tissue) and dislocation of brain structures develop. How dangerous a retrocerebellar cyst formed in the brain is depends on its size and location. Small cystic formations are often asymptomatic and do not cause discomfort to the patient.
The progressive growth of the cystic formation leads to compression of the surrounding brain structures, which causes disruption of its functions. It is incorrect to say that a cyst-shaped cavity of a certain size can be considered dangerous. The prognosis for each patient is made individually. In some cases, large cysts located away from vital centers of the brain do not cause neurological symptoms.
Conversely, a retrocerebellar cerebrospinal fluid cyst with a diameter of several millimeters can provoke hypertensive-hydrocephalic syndrome, the development of convulsions and epilepsy attacks, if it is located in such head regions as the trunk, medulla oblongata or cerebellum. Arachnoid forms localized in the area of the brain cisterns with a significant increase in diameter interfere with the circulation of cerebrospinal fluid, which leads to the development of hydrocephalic syndrome and increased intracranial pressure values.
Treatment
Special treatment is not carried out if:
- a brain cyst does not have severe symptoms;
- there is no growth in education;
- the size of the pathology is insignificant.
In such a situation, the patient is recommended to be under constant supervision of a neurologist and undergo preventive examinations at least once every six months to a year.
If the patient experiences the first signs of pathology, the benign formation begins to gradually or intensively increase in size, and there is increased fluid pressure inside the cyst, then surgical intervention is required.
Before performing surgery:
- The patient is given a thorough examination.
- Also, in parallel , the elimination of the cause that provoked the appearance and development of the cyst is carried out.
- Then specialists assess the risk of intervention and select the most optimal treatment option.
The method of surgical intervention depends on the location of the benign formation and its size.
In modern medicine, the following types of operations are distinguished:
- Endoscopic puncture. It is considered a modern method of intervention, which is the least traumatic. During the operation, an endoscope is used to pierce the skull. Afterwards, the formation is removed and the internal fluid is sucked out. It is used only in some cases, it all depends on the location of the cyst.
- Bypass surgery . Prescribed to a patient who has hydrocephalus and a constant flow of fluid.
- Neurosurgical operation , which is accompanied by craniotomy.
Causes
Primary cystic formations are congenital anomalies of brain formation, which are usually associated with adverse external influences on the fetus (intoxication, infectious diseases suffered by the mother during gestation, hypoxia, birth injuries) or hereditary predisposition. Causes of secondary forms:
- Past inflammatory processes and infections of the central nervous system (meningitis, encephalitis).
- History of surgical interventions in the brain area.
- Injuries, hemorrhages in the head area.
- Neurodegenerative processes.
- Cerebral blood flow disorders occurring in acute or chronic form (TIA, ischemia, cerebral infarction, stroke).
Statistics show that in 40-60% of cases after TBI, complications arise in the form of a cerebral cyst. Post-traumatic cystic formation can appear as a result of a concussion, compression or contusion of the brain of varying severity.
Retrocerebellar cyst of the brain in children and adults - what is it?
This brain pathology can occur in patients of different age groups. Timely diagnosis and treatment will help the patient avoid certain complications. In such a situation, it is not recommended to engage in self-treatment, since this is an ineffective method and can harm your health and provoke complications.
A retrocerebellar cyst of the brain is a bubble of a certain size that is filled with fluid. It appears in any part of the brain where, after a certain situation, the death of gray matter, an important component of this organ, is observed.
Previously, we wrote in detail about the causes of cysts in the head of a newborn baby.
This pathology also has another name - intracerebral cyst , since its formation occurs directly in the organ itself. Its danger lies in the fact that it occurs in the affected areas, which is not a normal phenomenon.
Therefore, when diagnosing the pathology, the cause of death of the gray matter will be clarified in parallel, in order not only to prevent further death, but also to prevent other complications.
Symptoms
The clinical course of a progressive cyst occurs in 3 stages - compensation, subcompensation, decompensation. At the 1st stage, the pathology is asymptomatic, at the 2nd stage, pronounced signs of damage to brain structures are observed, at the 3rd stage, the increasing development of hydrocephalus occurs. Symptoms of a retrocerebellar cyst of post-traumatic origin that forms in the head of an adult include cephalalgia and increased intracranial pressure. Other signs:
- Symptoms of damage to the cranial nerves (paresis, paralysis of the facial muscles, speech dysfunction due to impaired innervation of the organs of the speech apparatus, rarely oculomotor disorders).
- Transient short-term clouding of consciousness.
- Visual, auditory dysfunction.
- Motor dysfunction (impaired motor coordination, pyramidal insufficiency - increased skeletal muscle tone with the development of paresis and paralysis). In infancy, it manifests itself with a weak grasping reflex, tremor of the hands and chin, standing on tiptoes when walking (without support on the heel), throwing the head back.
- Deterioration of cognitive abilities.
- Behavior change.
- Convulsive, epileptic seizures are often of a generalized type.
- Astheno-neurotic syndrome (emotional lability, muscle and general weakness, deterioration in performance, irritability).
Disturbances in the functioning of the autonomic system are often observed - vegetative-vascular dystonia (dizziness, nausea, heart rhythm disturbances, increased heart rate, increased fatigue, sleep disturbance), sometimes accompanied by panic attacks. A retrocerebellar arachnoid cerebrospinal fluid cyst formed in the brain is manifested by symptoms:
- Feeling of pulsation and bursting in the area of the skull.
- Pain in the head area, resistant to drug therapy.
- Poor balance, difficulty keeping the body upright.
- Noise, hum, ringing in the ears, deterioration of hearing acuity.
- Disturbances in sleep and wakefulness (daytime sleepiness, nighttime insomnia).
- Fainting conditions.
- Deterioration of visual acuity.
- Paresthesia (skin sensitivity disorder - burning, itching, tingling sensation in the skin area).
In infants, signs are often observed: frequent regurgitation, bouts of vomiting, loss of appetite, crying for no reason, throwing the head back. In children of the 1st year of life, deformation of the bone structures of the skull, divergence of cranial sutures, and delayed mental and physical development are possible.
Diagnostics
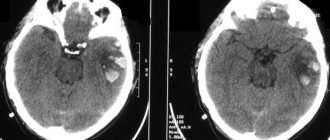
Diagnostic measures include collecting anamnesis, determining the somatic and neurological status of the patient. Consultations with a neurologist, otoneurologist, and ophthalmologist are indicated. Instrumental examination is carried out in the format of MRI and CT (neuroimaging); in parallel, EEG (electroencephalography) is prescribed to determine the bioelectrical activity of the brain and identify foci of epileptic activity.
Examination of newborn children is carried out using neurosonography. In doubtful cases, an MRI with contrast is performed. In the presence of a retrocerebellar cyst, an expansion of the cerebral-cerebellar cistern is often detected. Small cystic cavities that are asymptomatic often become an incidental finding during a diagnostic examination prescribed for another reason.
Treatment methods
Treatment of a retrocerebellar cyst formed in the brain of a child or adult is carried out taking into account its size and nature of its course. If the pathology is asymptomatic, therapeutic measures are limited to regular visits to a neurologist for observation. If neurological symptoms are present, medical or surgical treatment is performed.
Drug therapy
Drug treatment is carried out taking into account the symptoms and causes. If the formation of a cystic cavity is associated with an inflammatory process, antibiotics, antivirals, and immunomodulators are prescribed. Nootropic drugs and cerebral blood flow correctors improve blood supply to brain tissue, increase the energy status of neurons, regulate the processes of glucose utilization in nervous tissue, and activate synaptic transmission of nerve impulses. Anticonvulsants and antiemetics are prescribed if appropriate symptoms are present.
Surgery
Indications for neurosurgical surgery are divided into absolute and relative. In the first case, we are talking about such evaluation criteria as an increase in neurological deficit, hypertension syndrome (sustained increase in intracranial pressure values), provoked by a retrocerebellar arachnoid cyst or hydrocephalus, which developed against its background.
Relative indications include large cyst sizes, which cause deformation of adjacent parts of the brain, progressive growth of the cystic cavity, and disruption of the cerebrospinal fluid tract associated with the cyst. When considering the need for surgery, the individual characteristics of the patient are taken into account, for example, the elastic properties of brain tissue and the parameters of resorption (absorption) of cerebrospinal fluid. Contraindications to surgery:
- Gross disturbance of vital functions (cardiac, respiratory activity).
- Coma.
- Extreme physical exhaustion (in children).
- Acute inflammatory process.
The main surgical methods include microsurgical and endoscopic surgery, as well as bypass surgery. Surgical procedures are carried out under the control of intraoperative (continuous examination during surgery) ultrasound or neuronavigation.
Endoscopic intervention involves making a burr hole in the cranial bones, after which a cruciform opening of the dura mater is performed. The walls of the cyst are dissected, and a communication is created between the cystic cavity and the brain cisterns. The formed anastomosis with liquor ducts ensures the outflow of liquid contents, which leads to a reduction in the size of the cystic formation and elimination of the mass effect.
The microsurgical method involves performing a craniotomy - opening the skull to form a trepanation window through which access to the space-occupying lesion is provided. The dura is dissected linearly for the purpose of subsequent hermetically suturing of the hole. The wall of the cystic cavity is dissected and partially excised for histological examination.
Shunt operations are considered low-traumatic surgical methods. During the operation, a drainage system is installed, with the help of which the contents of the cyst are drained into a cavity located outside the skull. Implantation of a drainage system involves placing a catheter equipped with valves into the cystic cavity. The distal part of the drainage system is often placed in the abdominal cavity.
Etiology
A cyst can be either primary (congenital) or secondary (due to a disease).
In the second case, it is, in fact, a complication of the root cause.
Triggers can be:
- Deficiency of oxygen and microelements necessary for the brain;
- Consequences of surgical procedures;
- Stroke (ischemic and hemorrhagic);
- Inflammation of the meninges of an infectious nature (for example, meningitis, encephalitis);
- Open and closed craniocerebral injuries and mechanical damage (concussion).
- Impaired blood supply to the brain;
- Hereditary pathologies of connective tissue structure.
IMPORTANT! A retrocerebellar arachnoid cyst can form during fetal development or during difficult childbirth.
Possible complications
A retrocerebellar cyst is a formation that can be large in size and clinically dangerous in location, which is associated with difficulties in treatment. Common complications:
- Ineffectiveness of therapy (medical, surgical).
- Formation of liquor-type hydromas (secondary cystic formation).
- Formation of intracranial hematomas with subsequent development of cerebral edema.
- Decompensation of impaired circulation of cerebrospinal fluid.
Early postoperative complications include liquorrhea (leakage of cerebrospinal fluid), necrosis (tissue death) of the edge of the skin flap, and dehiscence of the surgical wound. Late complications include infectious lesions associated with the penetration of viral or bacterial agents into the wound.
Cystic retrocerebellar expansion is a formation most often located in the brain space behind the cerebellum. Symptoms of pathology depend on the size and exact location. It may be asymptomatic and then does not require treatment. In the presence of severe, progressive neurological symptoms, surgical intervention is usually performed.
201