Choroid plexus cyst in fetus and adult: causes, symptoms
Choroid plexus cyst (CPC) in the fetus and newborn is an ultrasound term formed due to excess accumulations of cerebrospinal fluid along the vessels. In most cases, as the baby grows, the formations go away on their own. If the structures are preserved, they do not pose a danger to the child's health. If the structures are preserved, they do not pose a danger to the child's health. Only in rare cases is surgery required to remove an overgrown cystic cavity.
The optimal period for diagnosing formations is the fetus at 18-22 weeks, when the structure of the brain is formed. Repeated ultrasound at 24-28 weeks notes a decrease in the number of cystic cavities.
Choroid plexus cyst in the fetus - what is it?
CSS is dangerous in children with chromosomal abnormalities such as Edwards disease (trisomy 18). The nosology is characterized by multiple malformations, so intracerebral cavities with cerebrospinal fluid are a minimal problem in treatment.
Down's disease is not characterized by the formation of the cerebral coronary artery system.
Interesting facts about choroid plexus cysts in children:
- Spontaneous disappearance in 90% of fetuses by 28 weeks of development;
- The prevalence rate of nosology among pregnant women is 2%;
- The shape, size, number of cavities varies;
- Found in adults and healthy people;
- The frequency of villous and choroid plexus cysts is about 3%.
It is impossible to determine the initial type of formations in the fetus due to physiological degradation. The absence of pronounced symptoms does not allow doctors to accumulate enough information about the pathology.
Morphological structure of choroid cystic cavities in a child
The accumulation of cerebrospinal fluid inside the choroidal formations does not pose a threat to the health of the baby. Morphologically, the cavity is represented by a thin wall, capable of changing size and shape.
Vascular plexuses are early structures in the formation of the central nervous system of the fetus. Bilateral localization is due to the presence of two hemispheres that require the content of cerebrospinal fluid. Scientists were unable to explain the need for the formation of limited cavities around the plexuses. Presumably, the structures are part of the formation of the central nervous system, and therefore disappear by 28 weeks. If development slows down, CSS can be observed in newborns, infants 3 months and somewhat older.
Cystic cavities of the brain are sometimes observed in adults. The pathology does not produce clinical symptoms, so they are detected by chance on an MRI performed due to the verification of another etiology.
Practice shows that there is no health hazard in the persistence of choroid plexus cysts after 30 weeks, with the exception of Edwards disease.
Causes of CSS
The etiology has not been established. It is considered likely that cystic cavities will persist for a long time against the background of viral infections, herpes, or complicated pregnancy. The absence of clinical manifestations until the end of a person’s life indicates the absence of harm from the pathology. The formations require dynamic monitoring. Blind fontanelles in a child allow an ultrasound of the skull to be performed, and periodic MRI is recommended for adults.
Viral cysts can change: they grow, they degenerate. Dynamic observation determines the prognosis of consequences for a person with CSS.
Two different diagnoses should be distinguished: “fetal choroid plexus cyst” and “cerebral vascular cyst”. The first nosology is harmless, goes away on its own or persists without dynamics for many years. The second type is dangerous, as it sometimes provokes symptoms.
There is a definition of “pseudocyst”. On the screen of an ultrasound monitor, doctors can detect a cavity formed by physiological structures.
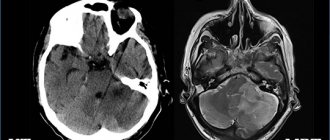
The exclusion of pathological conditions after the diagnosis of “choroid plexus cyst” in a newborn and fetus is ensured by an additional comprehensive examination. Genetic counseling rules out Edwards disease. Magnetic resonance imaging shows the structure of the soft tissues of the brain with high resolution, three-dimensional modeling of the area under study.
Detection of a choroid plexus cyst in a child requires verification of provoking factors: viral and bacterial infections, changes in the composition of the cerebrospinal fluid, increased intracranial pressure. If there are no additional changes, it can be argued that there are no conditions for the negative development of a vascular cyst.
My blog
I am writing for the sake of those who have encountered such a phenomenon as a choroid plexus cyst in the fetus.
Many ultrasound specialists, when they see this cyst, write in their conclusion simply a brain cyst. It sounds terribly creepy. It would be good if the doctor was competent and explained the essence of this problem. And if not, then tough luck. Sleepless nights, hysteria and tears are guaranteed. This is precisely why I am posting here, to reassure those faced with such a situation in advance.
I collided. We did an ultrasound at 19 weeks and saw this very “brain cyst”. I won’t describe my condition for a long time, despite the fact that the uzist woman’s question is where is it from? She only answered: this is due to infections (infections, by the way, are ureaplasma, which is not an infection per se). to the question, what to do now? go to the doctor, he will tell you.
On weak legs I made it to the doctor. She looked at the ultrasound again - yes, there is a brain cyst. Where did it come from, how to treat it and what will happen to the child, the answer is: “Well, most likely there will be no interruption, they give birth with this. Then a neurologist treats.” They gave me a referral to MONIIAG, to geneticists (also sounds scary). How does he treat it? Will the child be retarded, the reason for this? Not a single answer, complete confusion and ignorance. It’s good to have the Internet, I read articles and forums. I calmed myself down a little, tried not to cry, not to get nervous ahead of time. I survived the weekend and went to MONIIAG on Monday.
There they explained to me that it was not a brain cyst, but a choroid plexus cyst. There are often multiple cysts. They are formed at certain stages of brain development. They are not a congenital malformation (CD). Most likely, one of my small 6 mm tassels will resolve in 4 weeks; if not, it will resolve by 30-32 weeks, and if even then it does not resolve, then it will not have any effect on the child’s brain. The child develops normally, just like children without a cyst. The entire process of formation of such cysts and their resorption are explained in detail. I left full of confidence that everything would be fine and there would be no cyst at the control ultrasound.
Control ultrasound at 26 weeks. My doctor does it and the cyst is again... the same 6 mm. Again he gives a referral to geneticists.
I'm going there again. They do an ultrasound there and don’t see any cyst or other defects. There is no cyst, it has resolved, as they promised me.
So here it is for those who are looking for information on the Internet on this issue. The devil is not as scary as he is painted. Geneticists gave me all the answers to my questions. A choroid plexus cyst suggests that. that the child develops both hemispheres correctly. At 18-20 weeks, the brain begins to develop. Fluid (cerebrospinal fluid, that’s the name) accumulates between the choroid plexuses of the brain, forming sacs that look like a cyst on ultrasound. This is what they are called choroid plexus cysts. They often come in several pieces and reach quite large sizes. I had a 6 mm, small one. It happens up to 20 mm. Then after 24 weeks the brain begins to grow and the fluid simply goes away, the cysts resolve.
As I already said, this does not have any effect on the child’s brain and its development. CSS has nothing to do with infections; antibiotic treatment has nothing to do with it. These are the words of geneticists.
And I myself, having scoured the Internet thoroughly, came to the conclusion (maybe erroneous)) that this kind of thing is increasingly happening to boys (it’s true that girls also came across it). Almost all mothers who gave birth either with a cyst or after such a diagnosis boast, on the contrary, of a more developed child than peers without such a diagnosis (I probably want to think so, but let there be such a conclusion. By the way, I am a week ahead of my due date ))))) . Doctors prescribed antibiotics for many (I already said that genetics are against it). Many doctors attributed this to a lack of oxygen. There was also this option: the child is in a breech position, the blood flow is impaired. We need to turn it over somehow))) (I have a breech boy, by the way) And lastly, I haven’t found a single bad outcome on the internet. The cysts always resolved!
There is an article on this topic https://art.russ-med....3_russ-med.html
I hope my writing will be useful to someone. This is exactly the kind of feedback I have been missing about this issue. If you encounter this, don’t be nervous, don’t worry. Your baby feels everything and is afraid with you! But this problem is not worth it!
Choroid plexus cysts of a newborn baby
Detection of CSS after birth is not a dangerous condition, but requires examination of the newborn baby. Herpetic infection is activated when the immune system is weakened and can cause changes in the choroid plexus. As the baby grows, the immune system strengthens, so after 3 months, active development of immunity is observed. A decrease in viral activity stabilizes the condition. Cystic cavities can be observed in infants in the absence of clinical pathology. According to the standard scheme, children are examined three times:
- 3 months;
- 6 months;
- 12 months.
The absence of progression indicates the absence of changes that will contribute to the development of dangerous conditions.
Left choroid plexus cyst in a child
The choroid plexus is formed in the fetal body quite early. Education takes part in the formation of cerebrospinal fluid, which provides nutrition to the brain.
The diagnosis of left plexus cyst is common in newborns, although bilateral localization is more common. Pathology develops before the age of 1 year, when intrauterine infections are present. Cystic cavities are equally likely to form in any part of the brain.
Choroid plexus cyst of the right lateral ventricle
The nosology is considered the most benign, since most variants disappear on their own. Found after 22 weeks. An ultrasound scan after 28 weeks shows no pathology. The cystic cavity of the right ventricle can resolve. If there is no associated pathology (with damage to other ventricular spaces), this location of the cyst will not cause complications throughout life, even if the nosology persists in the child after 1 year. In adults, the nosology is rare.
Bilateral choroid plexus cysts
The pathology can persist into adulthood. Some cavities disappear, some remain. Despite the bilateral location, no clinical symptoms occur. Dynamic observation can reveal an increase in size and a change in shape. Only then is conservative treatment carried out. Chromosome mutations are preliminarily excluded. Geneticists can identify a genetic predisposition to Edwards disease. True, pathology can be determined without consulting on the external symptoms of the nosology, characterized by multiple malformations.
Ultrasound examination every 3 months allows you to monitor the condition of the brain parenchyma in infants. The procedure is sufficient to obtain information about the degradation or progression of cystic cavities.
Small cystic cavities in a child's brain
The nature of the CSS has not been reliably established. The pathology is an incidental finding. Small lesions do not affect the human psyche or metabolic reactions. There is no metabolic disorder, so there is no danger.
Small plexus and vascular cysts should be differentiated. The latter option provokes some symptoms. There is no threat to life or health. In adults, minor hemorrhages may occur, soaking into surrounding tissues.
Intrauterine infection provokes inflammatory damage to the walls of the cavity. Detection of infection requires the prescription of antibacterial drugs.
Detection of a plexus cyst at 19 or 20 weeks is not a reason for parents to worry. A repeat examination at week 29 will show no cavities.
Most scientists consider a cystic plexus of intracerebral vessels to be normal. The absence of a clinic suggests that the nosology is a variant of the norm. Improvements in diagnostic methods have made it possible to detect the disease in fetuses and infants more often.
You should pay attention to late cyst formation, which is the result of infection with herpes and a number of other viruses.
Possible symptoms and treatment
A brain cyst resulting from a hematoma, stroke, or aneurysm is one of the options for the outcome, which is generally favorable and is sometimes discovered only posthumously, however, along with a cyst formed as a result of a viral infection, it can sometimes have undesirable consequences, manifested by:
- Signs of hypertension in newborns;
- Feeling of compression of the brain;
- Some visual and/or hearing impairments;
- Minor motor coordination disorders;
- Epileptic seizures, which, of course, can be considered the most serious complication.
Clinical manifestations indicating the presence of a cystic formation occur in cases where the cyst compresses neighboring tissues and interferes with their normal functioning, that is, if it is of significant size or “settled” in unacceptable proximity to important centers of higher nervous activity.
In most cases, a brain cyst, like a choroid plexus cyst, does not require special treatment, however, if immunological studies have proven the presence of herpetic, cytomegalovirus or other infection, then treatment directed at the virus is indicated. In the presence of epileptic seizures, the patient is prescribed anticonvulsants, and, if necessary, surgical intervention is performed to eliminate the source.
If the symptoms are mild, but the patient occasionally complains of vascular manifestations of the cyst (dizziness, compression headaches, etc.), he is prescribed medications such as cinnarizine or Cavinton , which are well tolerated by the patient, improve blood supply to the brain and help normalize well-being.
Symptoms of choroid plexus cysts
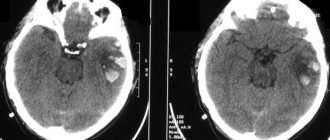
A brain cyst in adults can be a consequence of a hematoma. Limited accumulation of blood (subdural, epidural) with penetration into the ventricles of the brain contributes to ventricular cyst formation.
Pathology contributes to the appearance of clinical symptoms:
- Dizziness, headache;
- Movement coordination disorder;
- Muscle cramps, epilepsy;
- Hypertonicity in newborns.
Localization of manifestations near important nerve centers contributes to the emergence of specific symptoms.
The presence of cytomegalovirus or herpetic infection complicates the course of the disease. Detection of a pathogen and CSS in an adult with a high degree of probability indicates a viral etiology of cystic cavities.
Microcyst of the choroid plexus of the right lateral ventricle rarely causes neurological disorders.
In children, vascular microcysts and larger formations are not accompanied by pathological symptoms. The International Classification of Diseases (ICD 10) does not classify nosology as a number of pathological conditions.
Symptoms of choroid papilloma
Clinical signs of choroidpapilloma mainly depend on the location of the pathological focus. When the tumor is located in the area of the lateral ventricles of the brain, symptoms associated with an increase in intracranial hypertension are observed. Among them: increasingly intensifying headaches, nausea and vomiting, a state of stupor, disorientation, and the development of hallucinations. Headaches are paroxysmal in nature and can be very intense, causing a state close to loss of consciousness. To alleviate his condition, the patient usually takes forced positions. An ophthalmological examination reveals congestion of the optic discs and visual impairment. Further development of the pathology leads to the appearance of convulsions, and paresis or paralysis is also observed. With choroidpapilloma of the third ventricle, patients complain of headaches with a certain position of the head. A frequent symptom is a violation of the visual analyzer, which is expressed as a violation of the boundaries of the visual fields. With choroidpapilloma of the fourth ventricle, patients report attacks of headaches during physical activity or even with a rapid change in body position, as well as during defecation, coughing, etc. Common symptoms for tumors of this localization are vomiting (it can occur both with severe pain and without pain), dizziness, and convulsions. In advanced stages of choroid papilloma, signs of a neurological disorder develop: lethargy, irritability, apathy, and a state of stupor.
Consequences of choroid plexus cysts
Complicated cystic formations cause specific manifestations:
- Hypertonicity of newborns;
- Neurological symptoms due to compression of brain structures;
- Epilepsy (muscle cramps);
- Slight loss of vision and hearing.
Magnetic resonance imaging will need to distinguish a true vascular cyst from a pseudocyst. The latter type is a variant of the physiological development of the brain, but the anatomical structure when examined by ultrasound resembles a cavity. Magnetic resonance imaging is an accurate study (informativeness is about 96%). The three-dimensional modeling mode will allow you to correctly verify the nosology.
Edwards syndrome can be detected by ultrasound by identifying abnormalities of the limbs and changes in internal organs. Additional diagnostic tests:
- Determination of the concentration of human chorionic gonadotropin;
- Blood chemistry;
- Analysis of amniotic fluid.
A special risk group is women aged 32 years and older with hormonal disorders.