Chronic fatigue syndrome and immune dysfunction
Chronic fatigue syndrome (CFS) is a post-infectious (ARVI) chronic disease, the main manifestation of which is unmotivated, severe general weakness, which takes a person out of active everyday life for a long time. Previously, this disease was defined as myalgic encephalomyelitis [5], chronic Epstein-Barr viral infection, etc., and even earlier (in 1869) as “neurasthenia” and “neurocirculatory asthenia” [2]. For a long time, the interpretation of this disease was controversial.
In the United States of America, an outbreak of the disease was first noted in 1984 in the small town of Incline Village, Nevada, by doctors P. Cheney and D. Peterson. At that time, the authors considered the Epstein-Barr virus to be the root cause of the epidemic, since the majority of patients had antibodies to the specified virus in their blood. Further research revealed antibodies to other viruses. The nature of the epidemic and the discovery of antiviral antibodies allowed the authors to define their theory of the occurrence of CFS as viral.
Thanks to the efforts of researchers from many countries around the world - Great Britain, Australia, Germany and, first of all, the USA, by 1988 the main diagnostic criteria for chronic fatigue syndrome were formulated [3]. Since the main targets of the disease are the central nervous system and the immune system, the name of the disease has changed to “chronic fatigue and immune dysfunction syndrome”, which more fully reflects the pathophysiological basis of the disease and emphasizes the difference between CFS and the natural illness of patients after acute and chronic illnesses or injuries. The syndrome is not limited to any geographic or sociodemographic groups. According to various authors, the incidence of CFS can range from 10 to 37 cases per 100 thousand population.
The criteria published in 1988, 1991, 1992 and 1994 are used to diagnose CFS. Center for Disease Control (USA), which include a set of large, small and objective criteria. The main diagnostic criteria are: 1) persistent fatigue and decreased performance (by at least 50%) in previously healthy people over the past six months; 2) exclusion of other causes or diseases that can cause chronic fatigue.
The minor symptomatic criteria of the disease include the following. The disease begins suddenly, as with the flu, with 1) an increase in temperature to 38°C; 2) sore throat, sore throat; 3) slight enlargement (up to 0.3 - 0.5 cm) and tenderness of the cervical, occipital and axillary lymph nodes; 4) unexplained generalized muscle weakness; 5) soreness of individual muscle groups (myalgia); 6) migrating joint pain (arthralgia); 7) periodic headaches; rapid physical fatigue followed by prolonged (more than 24 hours) fatigue; 9) sleep disorders (hypo- or hypersomnia); 10) neuropsychological disorders (photophobia, memory loss, increased irritability, confusion, decreased intelligence, inability to concentrate, depression); 11) rapid development (within hours or days) of the entire symptom complex.
The disease begins suddenly, as with the flu, with 1) an increase in temperature to 38°C; 2) sore throat, sore throat; 3) slight enlargement (up to 0.3 - 0.5 cm) and tenderness of the cervical, occipital and axillary lymph nodes; 4) unexplained generalized muscle weakness; 5) soreness of individual muscle groups (myalgia); 6) migrating joint pain (arthralgia); 7) periodic headaches; rapid physical fatigue followed by prolonged (more than 24 hours) fatigue; 9) sleep disorders (hypo- or hypersomnia); 10) neuropsychological disorders (photophobia, memory loss, increased irritability, confusion, decreased intelligence, inability to concentrate, depression); 11) rapid development (within hours or days) of the entire symptom complex.
Objective (physical) criteria are: 1) low-grade fever; 2) non-exudative pharyngitis; 3) palpable cervical or axillary lymph nodes (less than 2 cm in diameter). The diagnosis of CFS is established by the presence of 1 and 2 major criteria, as well as minor symptomatic criteria: 6 (or more) of 11 symptomatic criteria and 2 (or more) of 3 physical criteria; or 8 (or more) of 11 symptom criteria.
People of any age are susceptible to the disease, but it has been noted that women aged 25–49 years are affected more often than men. In some cases, the disease develops 2 years after the first attack. In most patients, chronic fatigue and other accompanying symptoms, having begun during the period of a flu-like illness, decrease somewhat after one or two weeks, but recovery does not occur. In the most severe cases, severe depression may begin, loss of concentration and severe physical weakness occur. Cases of spontaneous recovery have been described. However, most patients continue to suffer from cyclical diseases for many months or years.
When making a diagnosis of CFS, guided by the main criteria, you should pay special attention to the peculiarities of the course of this disease in each specific case. According to many researchers, with CFS there may be disorders of the gastrointestinal tract, kidneys, liver and heart, allergies and increased sensitivity to odors, medications, alcohol occur, sudden weight loss is observed without breaking the diet, sweating at night, photophobia, hair loss hair and more etc.
To correctly diagnose CFS, differential diagnosis is necessary with diseases of the endocrine system, rheumatic diseases, neurological diseases, hematological diseases, chronic systemic diseases, poisoning with heavy metals, drugs, alcohol and the effects of radiation. In addition, differential diagnosis should be carried out with a disease such as fibromyalgia (FM), in which chronic and multiple muscle pain, fatigue, sleep disorders and other symptoms similar to CFS are observed (Table 1).
Table 1. Comparison of the severity of characteristic signs in CFS and FM
| Sign | CFS | FM |
| Sudden onset | +++ | + |
| Significant weakness | +++ | ++ |
| Painful lymph nodes | +++ | – |
| Fever | +++ | – |
| Morning tension | ++ | +++ |
| Sleep disorders | ++ | +++ |
| Pharyngitis | ++ | + |
| Headache | +++ | ++ |
| Anxiety | ++ | + |
| Immune dysfunction | +++ | + |
| Neurohormonal dysfunction | +++ | +++ |
Speaking about the etiology and pathogenesis of the disease and the role of the immune system, it should be noted that there are several theories. According to Professor J. Goldstein, director of the Institute of Chronic Fatigue Syndrome (California, USA), the disease is caused by an as yet unidentified virus. This may be one of the herpes viruses (Epstein-Barr /EBV/, cytomegalovirus /CMV/, herpes virus types 1 and 2 /HHV-1, 2/, herpes virus type 6 /HHV-6/), Coxsackie A viruses or B, enteroviruses, etc., which is confirmed by a number of researchers [5]. J. Goldstein defines CFS as a multicausal disorder of neuroimmune mechanisms, which manifests itself in genetically predisposed individuals as a result of activation of the immune system by infectious agents and dysregulation of the central nervous system, mainly its temporo-limbic region. The limbic system not only takes part in regulating the activity of autonomic functions, but largely determines the “profile” of an individual, his general emotional and behavioral background, performance and memory, ensuring a close functional relationship between the somatic and autonomic nervous systems. A latent infection can lead to illness (i.e., turn on) when exposed to a number of possible stimuli: severe emotional stress, adverse environmental factors, intoxication, trauma, surgery, pregnancy, childbirth, etc. One of the possible ways of developing immune dysfunction in patients with CFS and multiple allergies is shown in the diagram.
Another theory assigns a major role to neuropsychiatric factors with a predominance of immunodysregulation. Neuropsychological disorders are recognized as one of the diagnostic criteria for CFS. G. Taerk et al. noted a significant increase in the frequency of depression among patients with CFS compared to the control group. Using generally accepted diagnostic methods, severe depression was detected in 16 out of 24 patients. In addition, 50% of patients with chronic fatigue had at least one episode of depression before the onset of CFS. I. Hickie et al found depression in 46% of patients with CFS. In 12% of them, episodes of depression preceded the onset of CFS. Scientists believe that depression, as a premorbid condition, occurs more often in patients with CFS than in control groups. This suggests a psychological predisposition to CFS.
The role of depression in the development of CFS is difficult to assess, since many somatic signs of primary depression coincide with those of CFS. Therefore, the physician must decide on a case-by-case basis whether a mental disorder is a cause or a component of CFS. It should be noted that some immunological changes have been described in depressed patients; they were mainly characterized by a decrease in cellular immunological parameters. Therefore, it can be assumed that, at least partially, immunological changes in CFS may be due to concomitant depression.
At the same time, according to a group of leading CFS researchers from the University of Washington, depression and other psychological problems associated with chronic fatigue are a result of this fatigue or immunological and psychological dysfunctions that occur independently.
Numerous data indicate that both quantitative and functional immunological abnormalities are observed in CFS [1, 6]. There are a large number of “triggers” that cause immunological reactions that involve different types of blood cells and small molecules such as interferon and interleukin. It can be assumed that in patients with CFS these mechanisms are impaired [7].
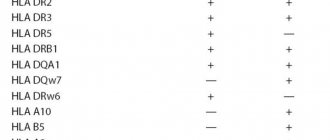
Currently, there are no laboratory tests that would clearly indicate the presence or absence of CFS in a patient [6]. Moreover, data provided by various researchers indicate the possibility of changing many indicators both upward and downward. For example, according to some sources [4, 7], 20% of patients with CFS have leukocytosis and the same number have leukopenia. Relative lymphocytosis is observed on average in 22% of cases (from 0% to 71% according to various sources) [6]. Australian researchers, on the contrary, found lymphopenia in 28% of patients. There is evidence that 30% of patients have atypical lymphocytes and in 48% of cases monocytosis is observed [6]. According to studies [7], on average, 31% of patients had a decrease in the level of serum immunoglobulins of classes A, D, G and M. IgD deficiency, mainly of subclasses G1 or G3, was present in 45% of the observed patients [8]. According to other materials, the level of immunoglobulins is increased in 28% of patients with CFS [7]. On average, 53% of patients had low levels of circulating immune complexes, while only 25% had reduced complement activity [6].
The manifestation of immune system dysfunction in patients with CFS was also expressed in a decrease in the cytological activity of natural killer cells; increased levels of interleukins 1-alpha, 2 and 6; reduction in the increased content of alpha-interferon and other cytokines in mitogen-stimulated lymphocytes; changes in the number and function of T- and B-lymphocytes [6].
| Immune dysfunction in patients with CFS |
It has been noted that in most patients with CFS, the disease is accompanied by allergic manifestations, including an increased skin reaction to a number of allergens and an increase in the level of circulating IgE. The mechanisms of this allergy have not yet been identified.
Serological tests usually do not reveal significant abnormalities. There is evidence of the presence of antinuclear antibodies and rheumatoid factor in low concentrations, but without clinical manifestations of systemic lupus or rheumatoid arthritis. Increases in cryoglobulins and cold agglutinins were found in a small number (8%) of patients.
The issue remains controversial regarding the detection of specific antiviral antibodies (HHV-6, EBV, CMV, Coxsackie, Herpes simplex). They are expected to be reactivated in patients with CFS. Enteroviruses can also serve as an etiological factor. Proponents of the viral etiology of the disease insist on a latent virus or viruses that are activated under certain conditions. One thing is clear that they have neuro- and immunotropic properties, since in CFS the central nervous system and the immune system are affected. Thus, changes in laboratory parameters in CFS are varied, sometimes contradictory, and often insignificant in degree. Despite this, there is no doubt that the functional state of the immune system has changed.
When diagnosing chronic fatigue syndrome and immune dysfunction on the basis of medical data and one’s own analysis, in addition to certain clinical and objective criteria, it is necessary to take into account a number of immunological indicators that are undoubtedly of important diagnostic value. They are summarized in table. 2.
Table 2. Immunological parameters for assessing CFS
| Options | Reduced | Norm | Promoted |
| 1. T helper cells | + | ||
| 2. T-suppressors | + | ||
| 3. TX/TS | + | ||
| 4. HLADR/CD8 (activated TC) | + | ||
| 5. CD38/CD8 (activated TC) | + | ||
| 6. CD3/CD56 (NK cells) | + | ||
| 7. CD56 (NK cells) | + | ||
| 8. Interleukin-2 receptor | + | ||
| 9. NK cell activity | + | ||
| 10. Mitogenic response of lymphocytes | + | ||
| 11. Humoral immunity | + | ||
| 12. Secretory IgA in saliva | + | ||
| 13. Immune complexes | + | ||
| 14. Tissue and protein antibodies | + | ||
| 15. Viral antibodies | + | ||
| 16. Fungal antibodies | + |
Attention should be paid to the fact that a number of changes in immunological parameters, namely a decrease in the functional activity of natural killer cells and macrophages, a decrease in the response of lymphocytes to mitogens and activation of CD+ lymphocytes, are common to CFS and various viral infections. That is why currently the most popular theory of the development of CFS considers the disease as a multicausal disorder of neuroimmune interaction, manifested in genetically predisposed individuals, probably under the influence of infectious agents (possibly viral in nature), leading to activation or imbalance of the immune system and dysregulation of the central nervous system. Since symptoms vary and may change with the use of neuropharmacological drugs, they may be mediated by neuroimmune transmitters. If we consider the neuroimmune system as a network (of interactions), it becomes clear that its work can be disrupted by factors affecting various parts of the system. Based on this, it would be logical to predict the success of treatment of CFS with psychotropic, immunomodulatory and anti-infective drugs.
Taking into account the latest data from foreign doctors, we can conclude that there is no specific treatment.
Certain treatment tactics have been developed that make it possible to prolong the remission of the disease and return patients to work [6]. Small doses of H2-blockers, tricyclic antidepressants and serotonin reuptake inhibitors (fluoxetine-Prozac) are used, which increase the patient’s energy capabilities, correct sleep, and reduce muscle soreness and tension. Symptomatic treatment is used, as well as vitamin therapy and physiotherapy. In each case, an individual approach is recommended. After leaving the hospital, patients remain in contact with their attending physicians, continuing to comply with a certain regimen and prescriptions [6]. The prognosis is favorable in most cases. Patients generally recover within 2 to 4 years, but full recovery of physical activity does not occur. Approximately 20% of patients experience a progressive increase in symptoms. Literature
1. Artsimovich NG //Theses of Symposium with International Participation Current Problems of Clinical and Experimental Psychoneuroimmunology. Tomsk, Russia, 1992. Vol. 1. P. 80 - 82. 2. Beard DS //Boston Medical and Suxgical J. 1869. Vol. 3. P. 217 - 220. 3. Bell DS, Bell KM //Ann. Intern. Med. — 1988. Vol. 109. No. 2. P. 167. 4. Bell DS //The CFIDS Chronicle. J. CFIDS Assoc. 1992. P. 2 - 5. 5. Bell EJ, McCarthey RA Riding MH//JR Soc. Med. 1988. Vol. 81. P. 329 - 331. 6. Buchwald D. //Post-viral Fatigue Syndrom. Edited by R. Jenkins and J. Mowbray. 1991. P. 117 - 136. 7. Buchwald D., Komaroff AL //Rev. Infect. Dis/ 1991 Vil. 13. Suppl 1. P. 12 - 18. 8. Buchwald D., Cheney PR, Peterson DL, et al.//Annals Inter. Med. 1992. Vol. 116. No. 2. P. 103 - 113. 9. Calabrese L., Danoa Th., Camera E., Wilke W. // The CFIDS Chrinicle. J. CFIDS Assoc. 1992. P. 6 - 12.
Chronic fatigue syndrome - symptoms and treatment
The intensive development of the information and social environment negatively affects the psychophysical state of a person, thereby provoking diseases previously unknown to science. One such disorder is chronic fatigue syndrome —a feeling of constant overwork.
The World Health Organization does not recognize this condition as a disease, however, the current International Classification of Diseases (ICD-10) contains similar symptoms, “Fatigue syndrome after a viral illness” (disease code - G93.3).[1]
Epidemiology
The prevalence of chronic fatigue syndrome among adults is 0.006–3%, but approximately 80% of all cases remain undiagnosed. The peak incidence of chronic fatigue syndrome occurs at the active age of 40–59 years. Women in all age categories are more susceptible to this disease and make up 60–85% of all cases [11].
Risk factors
Most often, chronic fatigue syndrome occurs in residents of megacities, since their rhythm of life and field of activity require constant psycho-emotional stress and multitasking. The risk group includes people who are engaged in professional growth, creating and supporting a family, solving many everyday issues, active relationships in society, and also bear an increased level of professional responsibility. All these factors lead to unbearable psycho-emotional stress and, as a consequence, nervous disorders and physical ailments - this is the stress-dependent hypothesis for the development of chronic fatigue syndrome.
A distinctive feature of chronic fatigue syndrome is the persistence of its main symptoms even after a long rest: neither a short-term change in activity nor departure from usual responsibilities can eliminate the root of the problem.
Etiology
The causes of the syndrome can be:
- unsatisfactory quality of lifestyle - intense daily rhythm, irrational time planning, prolonged mental or physical activity without breaks and rest (including lack of proper sleep, walks in the fresh air and change of environment);
- malnutrition - a lack of a balanced diet that includes vitamins and minerals that are essential for maintaining mental capacity, physical activity and emotional stability;
- diseases and ailments - chronic diseases, including psychological disorders, deplete the body’s resources, reducing its ability to recover and withstand stress;
- poor environmental conditions - a harmful environmental situation creates an unfavorable background for normal human life, therefore high levels of pollution and noise in cities lead to an increase in the number of the syndrome.