Service price
- HOSPITAL Day hospital5 000
- Day hospital with intensive care8,000
- 24-hour hospital (all inclusive, cost per day) 12,000
- 24-hour hospital (all inclusive, cost per day). Single occupancy24,000
- 24-hour hospital (all inclusive, cost per day). Single occupancy in a superior room 36,000
- Primary family counseling for relatives of patients undergoing inpatient treatment free of charge
- Group psychotherapy for relatives of patients undergoing inpatient treatment free of charge
- Group psychotherapy for 24-hour and day hospital patients free of charge
- Individual post for a hospital patient (if indicated)6,000
Paraphrenia is a fantastic delirium of “particularly large scope”, combined with increased (rarely decreased) mood. A more severe form of delusion than paranoia and paranoid.
Patients feel like rulers of people, planets and the Universe, centers of the struggle between good and evil, sources or conductors of divine forces. Paraphrenic syndrome is an indicator of a gross disruption of the brain and psyche.
Paraphrenia literally means “beside the mind” in Greek. It was first described by the famous German psychiatrist Emil Kraepelin in 1907 as a separate disease. However, to date, this is not considered a separate disease, but is a syndrome (a combination of several symptoms) that can develop in various mental disorders.
Complex of medical care
Only after a thorough diagnosis and establishment of an accurate diagnosis is an adequate course of treatment prescribed. The approach to each patient must be individual, based on the characteristics of the symptoms of the disorder.
Therapy can be carried out either on an outpatient basis or in a hospital setting. Only in the first case is it mandatory to regularly visit a medical facility to take the next dose of medication.
Aminazine is one of the popular drugs in the treatment of delusional disorders
Antipsychotics are most often used in treatment. They help get rid of increased anxiety, delusions and hallucinations.
Establishing the required dosage and duration of taking the drugs depends on the characteristics of the disease. In the acute form, an increased dose is prescribed during the period of increased clinical symptoms.
A chronic disease requires a minimum effective dosage with a gradual increase. In this case, medications are taken continuously.
Patients are most often admitted to the hospital in a severe stage of paraphrenia, when their behavior can become dangerous to others.
If a depressive state is diagnosed, additional courses of psychotherapy and antidepressants are prescribed.
Treatment of mental disorders has difficulties in establishing prognosis. According to statistics, only one person out of ten, after completing a full treatment course, gets rid of paraphrenic syndrome forever.
In other cases, relapses occur over time. However, after completing the next treatment course in combination with psychotherapeutic procedures, the symptoms disappear, which means the person can return to normal life without loss of ability to work.
It is worth noting that the pathology does not cause incurable changes in brain function, memory and thinking. The only exceptions are older people, for whom the likelihood of getting rid of this disorder is very low.
The following painful phenomena are characteristic of paraphrenia:
- A symptom of false recognition, when in unfamiliar people around them they see other, important persons participating in their lives.
- Fantastic delirium of grandeur.
- Increased mood (less often decreased), euphoria.
- Confabulations are false memories. The patient feels that he remembers certain events. However, in reality these events did not happen.
The causes of paraphrenia are gross disturbances of metabolic processes in the brain, overexcitation of subcortical structures.
Paraphrenic syndrome can be observed in the following diseases
- Organic mental disorders.
- Schizophrenia, schizoaffective disorder, other schizophrenia spectrum disorders.
- Atypical bipolar affective disorder.
According to the flow, acute and chronic paraphrenia are distinguished. Acute paraphrenia develops in a relatively short time and can be reversible. Chronic paraphrenia is difficult to treat and can last a lifetime.
To identify and make a diagnosis, the patient must be examined by a psychiatrist. Usually, a single examination by a doctor is enough to clarify the condition.
Treatment of paraphrenia should be carried out in a hospital. Therapy includes antipsychotic effects with drugs with anti-delirium action, and if ineffective, shock treatment methods. Other methods - physical therapy, psychotherapy, diet therapy - have an auxiliary effect.
As a rule, patients with paraphrenia, although not critical of their condition and not aware of their illness, do not resist hospitalization, perceiving what is happening as part of a “game” or performance that is played out around them. But in some cases they can resist and be aggressive. In these cases, involuntary hospitalization is required within the framework of Russian legislation.
If you encounter incorrect behavior in your loved one, do not waste time, contact a psychiatrist and arrange an examination of the patient. You can invite a psychiatrist to your home or go for a consultation yourself.
If you need help during hospitalization, contact us, we will help.
Paranoid syndrome. Paranoid syndrome
Paranoid syndrome. Primary systematized delirium of interpretation of various contents (jealousy, invention, persecution, reformism, etc.), occasionally existing as a monosymptom in the complete absence of other productive disorders. If the latter arise, they are located on the periphery of the paranoid structure and are subordinated to it. Characterized by a paralogical structure of thinking (“crooked thinking”) and delusional detailing.
The ability to make correct judgments and conclusions on issues that do not affect delusional beliefs is not noticeably impaired, which indicates catathymic (that is, associated with an unconscious complex of affectively colored ideas, and not a general change in mood) mechanisms of delusion formation. Memory disturbances in the form of delusional confabulations (“memory hallucinations”) may occur. In addition, there are hallucinations of the imagination, the content of which is associated with dominant experiences. As delirium expands, an ever wider range of phenomena becomes the object of pathological interpretations. There is also a delusional interpretation of past events. Paranoid syndrome usually occurs against the background of somewhat elevated mood (expansive delusions) or subdepression (sensitive, hypochondriacal delusions).
| | We will help you cope with paranoid syndrome! |
The content of delusions at distant stages of development can acquire a metallomaniac character. Unlike paraphrenia, delusion continues to be interpretive and in its scope does not go beyond the scope of what is fundamentally possible in reality (“prophets, outstanding discoverers, brilliant scientists and writers, great reformers”, etc.). There are chronic, existing for a number or even decades, and acute versions of paranoid syndrome. Chronic paranoid delusions are most often observed in relatively slowly developing delusional schizophrenia. Delirium in such cases is usually monothematic. The possibility cannot be ruled out that there is an independent form of the disease - paranoia.
Acute, usually less systematized paranoid states are more common in the structure of attacks of fur-like schizophrenia. The delusional concept is loose, unstable and can have several different themes or centers of crystallization of false judgments.
Some authors consider it justified to distinguish between paranoid and paranoid syndromes (Zavilyansky et al., 1989). Chronic, systematized, overvalued delusions (beginning with overvalued ideas) that arise under the influence of a key psychotraumatic situation for the patient are called paranoid. Paranoid and epileptoid features of the premorbid personality of constitutional, post-processual or organic origin contribute to the development of delusions. The mechanisms of delusion formation are associated with psychological rather than biological disorders - “psychogenic-reactive” delusion formation. Paranoid syndrome in this interpretation is appropriate to consider within the framework of pathological personality development.
Paranoid or hallucinatory-paranoid syndrome. Includes delusional ideas of persecutory content, hallucinations, pseudohallucinations and other phenomena of mental automatism, affective disorders. There are acute and chronic hallucinatory-paranoid syndromes.
| | Paranoid syndrome accompanies paranoid schizophrenia |
Acute paranoid is an acute sensory delusion of persecution (in the form of delusions of perception) of a specific orientation, accompanied by verbal illusions, hallucinations, fear, anxiety, confusion, and abnormal behavior reflecting the content of delusional ideas. It is observed in schizophrenia, intoxication, and epileptic psychoses. Acute paranoid states can also occur in special situations (long journeys associated with insomnia, alcohol intoxication, emotional stress, somatogenies) - road or situational paranoids, described by S.G. Zhislin.
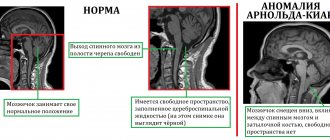
Acute hallucinatory-paranoid syndrome is an acute sensory delusion of persecutory content, arising against a background of fear, confusion and combined with pseudohallucinations and other phenomena of mental automatism. It is more common in the structure of attacks of fur-like schizophrenia, with atypical alcoholic psychoses. Chronic hallucinatory-paranoid syndrome (synonyms: Kandinsky-Clerambault syndrome, other eponyms, mental automatism syndrome, invasion syndrome, deposition syndrome, xenopathic syndrome, parasitism syndrome, influence syndrome, external influence syndrome, alienation syndrome, mastery syndrome, polyphrenia, nuclear syndrome) — the difference in names reflects the difference in the opinions of their authors regarding which disorders should be considered determining the structure of the syndrome: mental automatisms, disorders of self-awareness, the experience of openness or delusional ideas of physical and mental influence.
Mental automatisms in their completed form represent the experience of violence, invasion, the doneness of one’s own mental processes, behavior, and physiological acts. The following types of mental automatisms are distinguished.
Associative or ideational automatism - disorders of mental activity, memory, perception, affective sphere, occurring with the experience of alienation and violence: influxes of thoughts, non-stop flow of thoughts, states of blockade of mental activity, symptoms of investing, reading thoughts, symptom of unwinding memories, pseudohallucinatory pseudomemories, sudden delays memories, the phenomenon of figurative mentalism, etc.
Manifestations of ideational automatism also include auditory and visual pseudohallucinations, as well as a number of affective disorders: “induced” mood, “induced” fear, anger, ecstasy, “induced” sadness or indifference, etc. This group of automatisms includes “ made” dreams. The inclusion of auditory verbal and visual pseudohallucinations in the group of ideational automatisms is due to their close connection with thinking processes: verbal pseudohallucinations with verbal ones, and visual ones with figurative forms of thinking.
Senestopathic or sensory automatism is a variety of senestopathic sensations, the appearance of which patients associate with the influence of external forces. In addition, this includes olfactory, gustatory, tactile and endosomatic pseudohallucinations. Sensory automatism includes various changes in appetite, taste, smell, sexual desire and physiological needs, as well as sleep disturbances, autonomic disorders (tachycardia, excessive sweating, vomiting, diarrhea, etc.), “caused,” according to patients, from the outside.
Kinesthetic or motor automatism - impulses to activity, individual movements, actions, deeds, expressive acts, hyperkinesis that arise with the experience of violence. Receptive processes can also occur with the phenomena of being made: “They force you to look, listen, smell, look with my eyes...”, etc.
Speech motor automatism - phenomena of forced speaking, writing, as well as kinesthetic verbal and graphic hallucinations.
The formation of mental automatisms occurs in a certain sequence. At the first stage of development of ideatorial automatism, “strange, unexpected, wild, parallel, intersecting” thoughts appear, alien in content to the entire structure of the personality: “I never think like that...” At the same time, sudden interruptions of necessary thoughts may occur. Alienation concerns the content of thoughts, but not the process of thinking itself (“my thoughts, but very strange ones”).
Then the feeling of one’s own thinking activity is lost: “Thoughts float, go on their own, flow non-stop...” or states of blockade of mental activity arise. Subsequently, the alienation becomes total - the sense of belonging to one’s own thoughts is completely lost: “Thoughts are not mine, someone is thinking in me, other people’s thoughts are in my head...” Finally, a feeling arises as if thoughts “come from the outside, are introduced into the head, are invested... “Telepathic contacts with other people arise, the ability to directly read the thoughts of others and mentally communicate with others appears. At the same time, patients may claim that at times they are deprived of the ability to think or that they are “pulled out of thoughts” or “stolen.”
The development of verbal pseudohallucinations can occur as follows. First, the phenomenon of the sound of one’s own thoughts arises: “Thoughts rustle and sound in the head.” Then your own voice begins to be heard in your head, “voicing”, and sometimes like an “echo”, repeating your thoughts. This can be called inner speech hallucinations. The content of statements gradually expands (statements, comments, advice, orders, etc.), while the voice “doubles, multiplies.”
Then “other people’s voices” are heard in my head. The content of their statements is becoming more and more diverse, divorced from the reality and personality of the patients. In other words, the alienation of the process of internal speaking also increases in a certain sequence. Finally, the phenomenon of “made, induced voices” arises. The voices speak on a variety of topics, often abstracted from personal experiences, sometimes reporting absurd and fantastic information: “The voices behind the ears speak about local topics, but in the head they speak about national ones.” The degree of alienation of what is said by voices can therefore be different.
The dynamics of kinesthetic automatism generally correspond to those described above. At first, previously unusual impulses to action and impulsive desires appear, and strange and unexpected actions and actions are performed for the patients themselves. Subjectively, they are perceived as belonging to one’s own personality, although unusual in content. There may be short stops of action. Subsequently, actions and deeds are performed without a sense of one’s own activity, involuntarily: “I do it without noticing it, and when I notice it, it’s hard to stop.” Conditions of blockade or “paralysis” of impulses to action arise.
At the next stage, activity proceeds with a clear experience of alienation of one’s own activity and violence: “Something is pushing from within, prompting, not a voice, but some kind of internal force...” Episodes of interruption of action are also experienced with a tinge of violence. At the final stage of development of motor automatisms, a feeling appears that motor acts are done from the outside: “My body is controlled... Someone controls my hands... One hand belongs to my wife, the other belongs to my stepfather, my legs belong to me... They look with my eyes...” The states of blockade occur with a feeling of external influence. incentives to action.
The sequence of development of speech motor automatisms may be similar. At first, individual words or phrases are broken out, alien to the direction of the patient’s thoughts, absurd in content. Often individual words are suddenly forgotten or the formulation of thoughts is disrupted. Then the feeling of one’s own activity that accompanies speech is lost: “The tongue speaks on its own, I’ll say it, and then the meaning of what was said comes through... Sometimes I start talking...” Or the tongue stops for a short time and does not listen. Next, a feeling of alienation and violence arises in relation to one’s own speech:
“It’s as if it’s not me who speaks, but something in me... My double is using the language, and I’m not able to stop the speech...” Episodes of mutism are experienced as violent. Finally, a feeling of external mastery of speech arises: “Strangers speak my language... They give lectures on international topics in my language, and at this time I don’t think about anything at all...” Conditions of loss of spontaneous speech are also associated with external phenomena. The development of speech motor automatisms can begin with the appearance of kinesthetic verbal hallucinations: there is a feeling of movement of the articulatory apparatus corresponding to speech, and the idea of involuntary mental pronunciation of words. Subsequently, the internal monologue acquires a verbal-acoustic connotation, and a slight movement of the tongue and lips appears. At the final stage, true articulatory movements arise with the actual pronunciation of words out loud.
Senestopathic automatism usually develops immediately, bypassing certain intermediate stages. Only in some cases, before its appearance, can one state the phenomenon of alienation of senestopathic sensations: “Terrible headaches, and at the same time it seems that this is not happening to me, but to someone else...”
In the structure of mental automatisms, Clerambault distinguished two types of polar phenomena: positive and negative. The content of the former is the pathological activity of any functional system, the latter is the suspension or blockade of the activity of the corresponding system. Positive automatisms in the field of ideation disorders are a violent flow of thoughts, a symptom of investing thoughts, a symptom of unwinding memories, made emotions, induced dreams, verbal and visual pseudohallucinations, etc.
Their antipode, that is, negative automatisms, can be states of blockage of mental activity, a symptom of withdrawal, pulling out thoughts, sudden loss of memory, emotional reactions, negative auditory and visual hallucinations that arise with a feeling of accomplishment, forced deprivation of dreams, etc. In the field of senestopathic Automatism will be, respectively, sensations made and an externally caused loss of sensitivity; in kinesthetic automatism - violent actions and states of delayed motor reactions, taking away the ability to make decisions, blocking impulses for activity. In speech motor automatism, the polar phenomena will be forced speaking and sudden speech delays.
According to Clerambault, schizophrenia is more characterized by negative phenomena, especially if the disease begins at a young age. In fact, positive and negative automatisms can be combined. Thus, forced speaking is usually accompanied by a state of blockade of mental activity: “The tongue speaks, but at this time I am not thinking about anything, there are no thoughts.”
Disorders of self-awareness that arise in the syndrome of mental automatism are expressed by the phenomena of alienation of one’s own mental processes, the experience of the violence of their course, dual personality and the consciousness of an internal antagonistic double, and subsequently - a feeling of mastery by external forces. Despite the seemingly obvious nature of the disorder, patients usually lack a critical attitude towards the disease, which, in turn, may also indicate a gross pathology of self-awareness. Simultaneously with the increase in the phenomena of alienation, the devastation of the sphere of the personal Self progresses.
Some patients even “forget” what it is, their own Self; the old Self-concept no longer exists. There are no mental acts emanating from the name of one’s Self at all; this is a total alienation that has spread to all aspects of the inner Self. At the same time, thanks to appropriation, a person can “acquire” new abilities and characteristics that were not previously inherent in him. Sometimes the phenomenon of transitivism is observed - not only the patient, but also others (or mostly others) are the object of external influence and various kinds of violent manipulation, their own feelings are projected onto others. Unlike the projection itself, the patient is not subjectively freed from painful experiences.
The experience of openness occurs with the appearance of various echo symptoms. A symptom of echo thoughts - those around him, according to the patient, repeat out loud what he was just thinking about. Hallucinatory echo - voices from outside repeat, “duplicate” the patient’s thoughts. A symptom of the sound of one’s own thoughts is that thoughts are immediately repeated, they clearly “rustle, sound in the head, and are heard by others.” Anticipatory echo - voices warn the patient what he will hear, see, feel or do after some time. Echo of actions - voices state the actions, intentions of the patient: “I am being photographed, my actions are being recorded...” It happens that the voices are read for the patient, but he only sees the text.
Voices can repeat and comment on motives and behavior, give them one or another assessment, which is also accompanied by the experience of openness: “Everyone knows about me, nothing remains to myself.” Echo of writing - voices repeat what the patient is writing. Echo of speech - voices repeat everything the patient said out loud to someone. Sometimes the voices force or ask the patient to repeat for them what he told others, or, on the contrary, to mentally or out loud say again what he heard from someone, and the patient, like an echo, repeats this. The “hallucinatory personality” here seems to be deprived of contact with the outside world, establishing it with the help of the patient.
There is no name for this symptom, but we will conditionally call it the echo-patient phenomenon. The above echo phenomena can be iterative in the form of multiple repetitions. Thus, a patient (he is 11 years old) has episodes that last two to three hours, when what was said by other people three to five times in someone else’s voice is repeated in his head. One word is repeated more often. During repetitions, he perceives what is happening worse and cannot watch TV. Other echophenomena occur. Thus, the speech of others can be repeated by voices from outside or in the head - a symptom of echo-alien speech.
Voices with external projection are sometimes duplicated by internal ones - a symptom of echovoices. The experience of openness can also be observed in the absence of echo symptoms, arising in the most direct way: “I feel that my thoughts are known to everyone... There is a feeling that God knows everything about me - I am in front of him like an open book... The voices are silent, which means they are eavesdropping on what I think "
Delusion of physical and mental influence - a belief in the influence on the body, somatic and mental processes of various external forces: hypnosis, witchcraft, rays, biofields, etc.
In addition to the above-described phenomena of alienation, in the syndrome of mental automatism, opposite phenomena may occur - the phenomena of appropriation, which constitute an active or inverted version of the Kandinsky-Clerambault syndrome. In this case, patients express the belief that they themselves have a hypnotic effect on others, control their behavior, are able to read the thoughts of other people, the latter have turned into an instrument of their power, behave like dolls, puppets, parsleys, etc. Combination of alienation phenomena and assignments V.I. Akkerman (1936) considered a sign characteristic of schizophrenia.
There are hallucinatory and delusional variants of mental automatism syndrome.
In the first of them, various pseudohallucinations predominate, which is observed mainly during acute hallucinatory-delusional states in schizophrenia, in the second - delusional phenomena that dominate in chronically ongoing paranoid schizophrenia. In chronic schizophrenic delusions of the interpretative type, associative automatisms come to the fore over time. Senestopathic automatisms may predominate in the structure of attacks of fur-like schizophrenia. In lucid-catatonic states, kinesthetic automatisms occupy a significant place. In addition to schizophrenia, phenomena of mental automatism can occur in exogenous-organic, acute and chronic epileptic psychoses. Back to contents