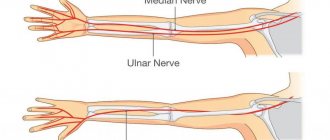
The radial nerve is a structure of mixed fibers. It starts from the cervical plexus and goes towards the hand.
Responsible for the innervation of the arm, flexion movements of the hand and skin sensitivity.
If it is damaged and left untreated, a person is deprived of the ability to act with this limb, to make subtle movements with the hand and fingers. This leads to disability.
The article discusses what radial neuritis is, how it manifests itself, and how it is treated.
What is it and the ICD-10 code
Radial neuritis is an inflammatory pathology that affects the nerve fiber itself and its sheath. Its ICD-10 code is (G56.3) .
Nerve damage is often caused by pinching. This is accompanied by pain, loss of motor function of the arm in the forearm, shoulder and hand with decreased skin sensitivity.
The arm stops bending at the wrist and elbow joints . Its frequent development is facilitated by the anatomical features of the location of this nervous structure.
These include:
- spiral course of the nerve trunk;
- close to the surface of the skin.
Thanks to this, it is easily and quickly affected by any adverse effects.
Causes of inflammation
There are several causes of damage to the radial nerve for the right and left arms.
These include:
- complications after an infectious disease, bacterial or viral;
- traumatic effect on the nerve fiber - this can be prolonged compression and disruption of blood supply due to an uncomfortable sleeping position, using a crutch or a tourniquet to stop bleeding;
- direct injury to the nerve due to injury or bruise, injection into the outer surface of the shoulder;
- compression of the nerve by a keloid scar formed after injury in the space between the muscles;
- toxic effects on nerve fibers from household and industrial toxic substances, carbon oxides, salts of heavy metals (lead, mercury).
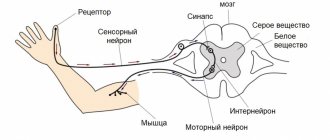
These reasons lead to disruption of the conduction of impulses along the nerve fiber of the radial nerve.
Symptoms and manifestations of damage
When the radial nerve is damaged, the patient loses fine motor skills of the hands, and movements in the hand are impaired. He cannot perform both complex and elementary actions with it. There is a loss of sensitivity or a decrease in it in characteristic areas.
Pain along the nerve trunk is extremely rare in patients. This only happens with infectious and traumatic lesions. The right upper limb is more affected.
Manifestations of neuritis of the radial nerve of the right and left hand depend on the location of the inflammation.
Depending on this, the following symptoms occur at different levels:
- With high nerve damage in the armpit area, paralysis of the extensor muscles of the fingers, hand and forearm is observed.
- For lesions in the middle third of the nerve trunk (at the level of the middle third of the shoulder), extension of the forearm and hand is typically affected. Movement in the shoulder is preserved.
- Damage to the nerve in the lower third of the shoulder is manifested by impaired flexion of the fingers and hand. All other movements in the arm (flexion of the weep and forearm) are preserved.
- If the nerve is damaged at the level of the lower part of the forearm, the ability to extend the fingers disappears or decreases. All other functions are retained. Patients develop a “dangling hand” typical of this nerve lesion. The thumb is pressed against the index finger. The patient is unable to shake hands and the fingers are fully extended.
Find out about the symptoms of other types of neuritis of the extremities:
- upper - brachial, ulnar, median nerves;
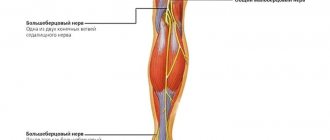
- sciatic nerve;
- lower - femoral, tibial and peroneal nerves.
Possible patient complaints
Patients present a variety of complaints of weakness in the arm, fingers and hand, and decreased range of motion. Their pain radiates or even shoots into the third, second and first fingers of the hand.
They complain of numbness in the affected hand, goose bumps in the fingers of the hand, except for the fourth and fifth, the outer side of the shoulder and the inner side of the forearm.
There is a violation of deep and superficial sensitivity in the area of the fingers (I-III) and forearm on the inside. The brush swells and acquires a bluish-purple color.
The patient notes a violation of the flexion of the wrist joint, the fingers do not straighten . Occasionally, numbness along the nerve trunk is possible.
results
In both cases under consideration, at the time of examination, the patients had the same clinical picture in the form of motor deficit in the muscles innervated by the MN for 3-6 months. The pain syndrome accompanying mononeuropathy was intermittent, unexpressed and not neuropathic in nature. No sensory disturbances were found.
The development of MN neuropathy in patients was preceded by intense stereotypical physical activity - flexion and extension of the arm at the elbow and wrist joints in combination with its pronation and supination.
Ultrasound revealed a hypoechoic increase in the MN in both cases considered compared to the opposite side (see figure).
Comparative characteristics of two clinical cases - a 64-year-old patient (left) and a 48-year-old patient (right). a - ultrasound image; b — intraoperative picture of compression of the deep branch of the radial nerve by the arterial branches of the recurrent radial arteries; c — 3D reconstruction of the anatomical situation. The different lengths of the altered portion of the nerve were noteworthy. In the 1st case - 7 mm with a distal sharp narrowing of the nerve at the level of 1 cm distal to the shadow of the joint space of the elbow joint; in the Color Doppler mode, the arterial trunk is visualized, located distal to the enlarged portion of the nerve, possibly causing compression of the spinal nerve. In the second observation, the length of the changed area was 15 mm with an uneven external contour, and in the Color Doppler mode, multiple dilated arterial trunks were revealed along the lower edge of the nerve.
Needle EMG in the presented observations revealed signs of denervation in the form of fibrillation potentials and positive sharp waves in the common extensor digitorum and extensor digitorum longus. An isolated lesion of the spinal nerve in the presence of an intact trunk of the common radial nerve is proven by the absence of neurophysiological changes in the extensor carpi radialis.
Both patients underwent surgery. The operations were performed from a standard projection approach and consisted of revision and decompression of the nerve. In the first observation, a posterior interosseous nerve was found with a tight arterial loop forming a “vascular noose” around the nerve. In the second observation, dilated arterial trunks ran close to the lower edge of the nerve, one of which, with a small diameter, enveloped the nerve in a “loop.” Another, larger one, pierced the nerve through and through (see picture). During the revision, the recurrent radial arteries are coagulated and divided, and the nerve is released. The postoperative period proceeded smoothly, the wounds healed by primary intention, a set of exercises was recommended to develop the fingers with an emphasis on the work of the extensors, and recommendations were given to limit excessive physical activity on the extension of the hands in the wrist joint.
When observed 1 month after surgical treatment, a decrease in the severity of motor deficit was noted, more in the common extensor of the fingers, to a lesser extent in the extensor of the fifth finger in both patients (see table),
Dynamics of changes in muscle strength in points on the MRC scale in 2 operated patients Note. Data are shown before (1) and after (2) surgical decompression of the nerve. BR—brachioradialis muscle; Sup - instep support; ECR—extensor carpi radialis; EDC—extensor carpi communis; EI - extensor of the fifth finger; EPL - extensor digitorum longus. the pain syndrome has regressed.
Diagnostic methods
A neurologist treats radial nerve neuritis . First, he asks the patient about complaints and medical history.
Finds out under what circumstances and when the signs appeared. Then the doctor proceeds directly to examining the patient. Based on this, he makes a preliminary diagnosis.
A neurological examination reveals:
- During examination of the patient's hand, a characteristic drooping hand is revealed when the arm is extended forward.
- Difficulties in bending joints are revealed. The patient does not straighten his hand, forearm, and his arm does not straighten at the elbow joint.
- When examined with a neurological hammer, the doctor detects a decrease in the carporadial and extensor reflexes.
- There is a violation of skin sensitivity in the area of the 1st, 2nd, and 3rd fingers.
- A series of tests are performed to determine the level of radial nerve damage. He cannot move his thumb to the side. The patient is unable to simultaneously touch the back of the hands with all fingers. He cannot place his palms on the table and cross his middle and second fingers. A patient with damage to the nerve trunk is unable to spread his fingers to the sides.
Tests and neurological examination data may suggest damage to the radial nerve. It can be confirmed by performing a series of instrumental studies.
Electroneuromyography plays a leading role in making a diagnosis. It allows you to determine a violation of the conduction of a nerve impulse along a nerve fiber and a defect in the innervation of certain muscle groups. There is a decrease in the amplitude of the muscle response to electric current stimulation.
They also conduct electroneurography , which reveals a slowdown in conduction along the nerve trunk.
In addition to these studies, additional testing is carried out. They are carried out to identify the cause of damage to the radial nerve.
These include:
- consultations with a traumatologist, orthopedist and endocrinologist;
- blood biochemistry;
- determine blood sugar levels;
- general blood analysis;
- radiography of the bones of the shoulder, forearm, hand;
- CT scan of the elbow and wrist joints.
What diseases should be distinguished from?
Differential diagnosis for neuritis of the radial nerve is carried out with neuropathy . It is characterized by all the same symptoms, but there is no pain syndrome.
Neuritis should also be distinguished from post-traumatic compression of the radial nerve . To do this, a hydrocortisone-novocaine blockade is carried out in the area of its membranes.
When the nerve fiber is compressed, relief of symptoms is observed, which is absent with neuritis.
Radial nerve neuropathy
13.03.2020
Neuropathy is a syndrome of "drop" hand. In this case, a person who suffers from this disease experiences difficulties in the flexion and extension functions of the hand, as well as problems with the index and thumb. With neuropathy, it is difficult to form a fist or move your thumb to the side. Pain, numbness, and burning appear in the place where the radial nerve passes.
The causes of radial nerve neuritis occur due to pinching of the nerve root. These problems can appear due to injuries, incorrect hand position during sleep or injection.
The main causes of radial nerve neuropathy
- Injuries. In this situation, neuropathy can occur with a fracture of the elbow, shoulder, or radius , where a piece of bone can damage or cut off a nerve.
- Infections. Nerves can be damaged not only by injuries, but also by infectious diseases, as well as viruses and bacteria that directly affect the nerve itself.
- Intoxication. Here we are talking about poisoning with poisons, heavy metals, alcohol and drugs.
- Physical exercise. Performing any complex and difficult physical exercises for the body can negatively affect a person’s health, that is, pinching of a nerve can occur.
- Squeezing. This can happen if the hand is positioned incorrectly during sleep, or if a tourniquet is applied incorrectly in case of severe bleeding or tumors, where the occurrence of any formation can put pressure on the nerve fibers and lead to numbness. Crutches can also become dangerous if used incorrectly.
The symptoms of this disease depend on the location of the injury. Pinching of the nerve process in the armpit most often indicates that the patient was using crutches incorrectly or that another person was lying on his arm while sleeping; this is otherwise called “sleeping” paralysis. Problems bending the elbow, hand and fingers can cause discomfort and serious problems. If the nerve damage occurred in the elbow joint, then the “dropping” hand syndrome is more pronounced. There is also pain and numbness in the wrist. All these problems can occur in people of any age. Therefore, if any signs appear, you should consult a doctor .
To make an accurate diagnosis, a neurologist will conduct a series of examinations. In addition to a visual examination, where the neurologist examines the patient’s medical history, past illnesses or injuries, the doctor checks the mobility of the hand and fingers, their sensitivity, and prescribes additional tests and diagnostics. After the causes and location have been found, a number of medications, physical therapy , current therapy and massage . The patient is under constant supervision of a neurologist , because treatment adjustments occur over time. Either a change in some pills and injections, or a change in procedures under the supervision of a competent specialist.
In order to avoid these problems, it is necessary to lead a healthy lifestyle. Exercising, eating right, taking vitamins, and giving up bad habits will help reduce the risk of the disease. Exceptions include injuries.
Published in Neurology Premium Clinic
Features of treatment
Treatment of the radial nerve is carried out only by a neurologist or a rehabilitation specialist. Self-medication is unacceptable. The limb must be immobilized during treatment.
Therapy has two goals. The first is treatment of the underlying disease or injury that led to the nerve damage. The second is the removal of symptoms: pain, swelling, sensory disturbances and decreased muscle strength. Its tactics are determined by the cause of the disease and the level of damage.
The following drugs are used:
- Non-steroidal anti-inflammatory drugs (Ibuprofen, Nimesulide) reduce hand swelling and nerve inflammation.
Angioprotectors are used to improve regional blood circulation and blood supply to the nerve trunk. Used: Actovegin, Pentoxifylline, Trental.- Anticholinesterase drugs (Prozerin) enhance the conduction of impulses along the nerve.
- B vitamins improve metabolism in nerve fiber.
For treatment, drugs high in vitamins B1, B6 and B12 are used. Vitamin complexes are used: Neuromultivit, Neurodiclovit and others. - To treat severe pain and swelling, I use glucocorticoids; they have anti-edema and anti-inflammatory properties.
- Antioxidants (Vitamin E, Vitamin C) reduce the severity of damage in the nerve fiber.
In the recovery period for neuritis , physiotherapy, electrical myostimulation, acupuncture, massage, and exercise therapy are prescribed .
Physical therapy plays an important role in the treatment of neuritis of this localization. A set of exercises is developed by a rehabilitation specialist for each patient.
The following exercises are used:
- The patient is seated at the table. He bends at the elbow joint and rests against the surface of the table. In this position, he raises his index finger up and lowers his thumb down. The exercise is performed ten times.
- In the same position, raise your thumb up and your index finger down. The exercise is performed ten times.
- Extend the fingers of the healthy hand ten times. Then grab the fingers of the affected hand into a fist with your healthy hand and squeeze ten times.
In rare cases, if there is no effect from conservative treatment, surgery is performed . With them, the nerve is released from compression.
How is radial neuropathy of the radial nerve treated?
The main direction in healing from neuralgia of this type is the elimination of the factors that caused it. A number of measures are carried out to maintain the metabolism and blood vessels of the area that has been subjected to destructive effects, and the functionality and strength component of muscle tissue are restored. In any case, an integrated approach to solving the problem is necessary. The treatment program includes drug therapy: taking antibiotics, anti-inflammatory and decongestant drugs. If necessary, the body is detoxified. In the case of traumatic neuralgia, the dislocation is reduced, the position of broken bones is corrected, and the limb is fixed. Often such injuries are so complex that corrective surgery, including nerve grafting, is necessary to eliminate them.
Vitamins B1, B6, hemodialysate, thioctic acid, pentoxifylline, nicotine, neostigmine contribute to faster recovery. Massage, manual therapy, electrical myostimulation, and physical therapy are also recommended.
Prognosis and prevention
Radial neuritis responds well to treatment in young people . In the elderly, neuritis, in the presence of concomitant diseases, is difficult to treat. Complications develop quickly.
To prevent diseases, it is necessary to promptly treat the pathologies that cause them. Radiation neuritis is caused by a complex of causes.
With minimal manifestations of illness, numbness, or weakness in a limb, you should consult a doctor and follow all his prescriptions and recommendations .
Otherwise, paralysis and paresis occur, and disability develops. This significantly reduces the patient’s ability to work and quality of life.