Classification
Subdural hematomas are classified according to the speed of development of clinical signs. There are the following types of hemorrhages:
- acute subdural hematoma: manifestations occur within seventy-two hours from the moment of injury;
- subacute subdural hematoma is defined when symptoms develop within four to fourteen years after injury;
- chronic subdural hematoma is characterized by the onset of symptoms several weeks or months after injury (usually more than three weeks).
Subacute and chronic types of hemorrhages occur more often as a result of vascular damage under the influence of various factors; acute – as a result of traumatic brain injury. Subdural hemorrhage occurs with equal frequency both on the side of injury and on the opposite side according to the biomeanical principle of counter-impact (the brain is displaced to the side opposite to the impact and can be injured when colliding with the bone skull on the opposite side).
Diagnosis and treatment
To correctly diagnose the disease, specialists prescribe a number of tests, and it is especially important to do magnetic resonance imaging and computed tomography. Based on the results of the examination, a decision will be made on the need for hospitalization of the patient and the choice of an effective treatment regimen for chronic subdural hematoma of the brain. Most often, given the characteristics of the disease, there is no need to remove the entire hematoma, since it is enough to drain a third of the fluid through the trefination hole, and the remaining part will disappear on its own, but this should not take 1.5-2 months.
In addition to surgical intervention, there is the possibility of conservative treatment of the disease, but most often one cannot expect good results from such treatment. Conservative treatment involves the use of decongestants and drugs that improve blood circulation; drugs that improve metabolism, painkillers and antiemetics can also be prescribed. Rehabilitation after chronic subdural cerebral hematoma occurs in the intensive care unit, and recovery is better with good care, and the risk of re-hemorrhage is reduced by limiting physical activity.
Symptoms
The symptoms of a subdural hematoma are extremely variable. Manifestations of hematoma are caused by local, cerebral and brainstem disorders. A “light” period is characteristic - the time period immediately after the injury, when there are no manifestations. The duration of the “light” interval can vary from minutes and hours to several days. In chronic forms, this period can be months or years.
Subdural hematomas are characterized by an undulating course, while other patients may suddenly fall into a coma.
Focal symptoms depend on the location of the hemorrhage, general cerebral symptoms depend on its volume and the amount of compression of the brain, brainstem symptoms depend on the nature of the lesion in the brainstem and the percentage of its wedging into the foramen magnum.
Life forecast
The prognosis of life with chronic subdural hematoma depends on the timeliness of seeking medical help. Severe consequences are observed mainly in elderly patients. Lethal cases occur not only due to the presence of the hematoma itself, but also against the background of traumatic effects on brain tissue. Edema, cerebral ischemic processes, and dislocation of brain structures may occur.
After surgical treatment, it is necessary to establish strict monitoring of the patient's condition. In the first hours after surgery, cerebral edema may occur.
Surgery for chronic hematoma is one of the most effective treatment methods. Conservative therapy is used as an additional way to help the patient. The Medsi Clinic successfully performs neurosurgical operations for such conditions.
Variants of the course of the disease
There are three main variants of the clinical picture of subdural hemorrhages:
- Classic clinic. A change in the state of consciousness occurs in three phases: loss of consciousness at the time of injury, a clear “bright” interval, and repeated loss of consciousness. During the recovery period, the patient reports severe headaches, nausea, dizziness, and possible memory loss. Focal symptoms manifest themselves later, during the period of deepening stunning. At the same time, a sharp increase in headache occurs and vomiting develops.
Focal symptoms: most often these are mydriasis, sensitivity disorders, contralateral pyramidal insufficiency (lack of brain function appearing on the opposite side from the side of the lesion).
From stem symptoms
: secondary stem syndrome (decrease in heart rate, respiratory dysfunction, tonic convulsions).The three-phase clinical pattern is more common for the subacute form than for the acute form. In these cases, euphoria and decreased criticism of one’s condition may occur.
- Option with an erased picture of the “light” gap. Primary loss of consciousness can reach the level of coma. Stem and focal symptoms are clearly expressed. Then there is a partial restoration of consciousness (usually to the point of stunning). After some time, the patient again falls into stupor or coma, and the disturbances in vital functions deepen. Epileptic seizures may develop, and hemiparesis increases.
- Option without a “light” gap. Occurs with multiple, severe brain injuries. The patient is in a stuporous state or in a coma. Moments of clarity of consciousness are either erased or absent; there is practically no positive dynamics noted.
general description
Subdural hemorrhage (acute) non-traumatic (I62.0) is a sudden hemorrhage under the dura mater.
Prevalence: 12 per 100 thousand people. Occurs more often in men (70%) over the age of 40 years.
Risk factors for subdural hemorrhage are arterial hypertension, atherosclerosis, smoking, alcohol abuse, physical or emotional stress. Hemorrhage occurs against the background of cerebral vascular pathology, blood diseases, or taking medications that affect blood clotting.
Consequences of subdural hematoma
The occurrence of subdural hemorrhage is accompanied by rapid displacement of the brain and infringement of its stem structures. Subdural hematoma usually develops against the background of severe damage to the skull and brain, and therefore has an unfavorable prognosis.
The outcome and consequences of a subdural hematoma of the brain depend on the speed of recognition of the hemorrhage and the competently chosen treatment method. The prognosis is based on other factors: the patient’s age, the volume of hemorrhage, somatic complications. Statistics today indicate a high mortality rate among such patients and disability among survivors.
Symptoms and causes of hematomas
Chronic subdural hematoma can have different sizes, which determines, first of all, the treatment regimen and the percentage of positive outcome. Small hematomas up to 50 millimeters in size resolve as a result of drug treatment; treatment of medium-sized hematomas (up to 100 mm) becomes somewhat more complicated, and here much depends on the location of the source of the disease. Serious consequences most often occur with a large hematoma. By the way, in contrast to the acute phase, diagnosis of chronic subdural hematoma of the brain is rarely made, since the disease is quite rare.
Symptoms of chronic subdural hematoma of the brain appear only in the third week after injury, although this disease is often diagnosed in infants, but most often it is diagnosed in middle-aged and elderly people. As a rule, this is the result of an injury or blow to the head; such injuries are often caused by improper handling of the baby, for example, by throwing it up. As for the chronic form of the disease, it usually occurs with repeated head injuries. It is also worth mentioning predisposing factors of the disease, such as oncological tumors in the brain, problems with blood vessels, brain atrophy, inflammatory vascular diseases and even bad habits.
Surgery for chronic subdural hematoma is prescribed only after a study and face-to-face consultation with a neurosurgeon, and treatment of the disease, among other brain pathologies, is carried out at the Institute named after. Burdenko. The reason for contacting a medical facility may be headache and nausea - the first symptoms of CSH; severe vomiting and increased blood pressure often also occur.
Treatment
It is performed conservatively or surgically, depending on its type, volume, as well as the individual characteristics of the patient. In the acute form, removal of the subdural hematoma is often indicated. Detection of displacement and compression of brain structures is a stimulus for surgery as soon as possible from the moment of injury (or rupture of a vessel).
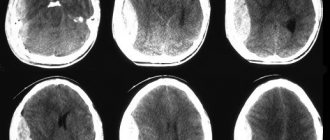
a) With MRI without contrast, the image reveals areas of fluid accumulation indicated by white arrows - subacute subdural hematomas. b) MRI visualizes foci of increased signal intensity (indicated by white arrows), as well as foci of reduced MRI signal intensity (indicated by black arrows), these signs are characteristic of acute subdural hematomas.
The absolute indication for surgical treatment of a subdural hematoma is the thickness of the accumulated blood more than one centimeter, determined by imaging studies (MSCT, MRI). The postoperative period should be accompanied by the maintenance of vital functions and control of intracranial pressure.
The operation is also indicated for subacute subdural hemorrhage, if there is an increase in focal symptoms and the appearance of signs of intracranial hypertension.
Methods for treating chronic subdural hematoma
For treatment of chronic subdural hematoma, surgical intervention is recommended. It is impossible to remove the resulting capsule using medications.
It is recommended to perform osteoplastic craniotomy as one of the types of minimally invasive neurosurgery. The formation with liquid must be emptied by 30 percent. After this, within 1.5-2 months the body will independently remove the remaining accumulated blood. Remains of CSH may be destroyed on their own after surgery. For this purpose, conservative therapy methods are not used.
If the patient promptly seeks help from a medical institution, the treatment prognosis is quite favorable. If help is provided late, there is a risk of irreversible brain damage. In the most difficult situations, death is also possible. This occurs either when the capsule enlarges too quickly, or when the patient continues to ignore his own symptoms.
Clinical picture
Symptoms appear simultaneously while you are awake. Simultaneously with the disturbance of consciousness, the symptoms of the disease increase over several hours and days. Subdural hemorrhage is characterized by sudden intense headache, vomiting, and weakness/numbness in one side of the body. Drowsiness or agitation, cramps in the limbs, decreased memory, and increased blood pressure may be expressed.
A neurological examination of the patient reveals psychomotor agitation (50%), impaired consciousness (80%), cerebral syndrome (90%), focal/generalized seizures (35%), homolateral mydriasis (40%), nystagmus (35%), ophthalmoplegia ( 15%), contralateral hemiparesis/hemihypesthesia (40%), amnesia (10%). Bradycardia is observed in 40% of cases, respiratory rhythm disturbances - in 20%.
How to treat subdural hematoma?
Treatment of subdural hematomas can be carried out using conservative and surgical methods. The choice of tactics is determined individually, taking into account the volume of the hematoma, the phase of its development and the patient’s condition.
The absolute indications for surgical treatment of subdural hematomas are:
- acute subdural hematoma, causing compression and displacement of the brain; the sooner the subdural hematoma is removed, the more favorable the prognosis for recovery;
- subacute subdural hematoma with increasing focal symptoms and/or signs of intracranial hypertension.
Any other circumstances may be grounds for surgery only at the discretion of the attending physician, taking into account the totality of clinical and radiological data.
Drug treatment of subdural hematoma is relevant:
- for victims in clear consciousness:
- if the hematoma thickness is less than 10 mm,
- when the midline structures are displaced by no more than 3 mm,
- without compression of the basal cisterns;
Resorption of a planar subdural hematoma usually occurs within a month.
In some cases, a capsule forms around the hematoma, which means the process becomes chronic. If dynamic observation indicates a deterioration in the patient’s condition or an increase in headaches, or congestion occurs in the fundus, this turns out to be an indication for surgical intervention, or more precisely for closed external drainage.