Neuromuscular diseases
This is a group of hereditary diseases that are transmitted at the genetic level (X-linked, autosomal dominant, autosomal recessive forms, maternally inherited mitochondrial forms). About a third of disease cases are the result of new mutations. Taking into account the structural organization, the following levels of damage to the neuromuscular system are distinguished:
- Primary muscular lesions (muscular dystrophy of Duchenne, Becker, myopathy, myotonia).
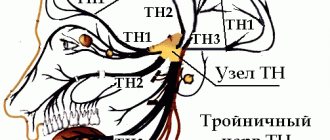
- Synaptic lesions (neuromuscular transmission disorders - myasthenia gravis).
- Neuronal lesions (spinal muscular atrophy).
What muscle diseases exist?
- Inflammatory myopathies.
- Infectious myopathies.
- Drug-induced and toxic myopathies.
- Secondary metabolic and endocrine myopathies
- Hypokalemic myopathy.
- Hypophosphatemic myopathy.
- Myopathy in chronic renal failure.
- Myopathy in diabetes.
- Myopathy in hypothyroidism.
- Myopathy in hyperthyroidism.
- Myopathy in hyperparathyroidism.
- Cushing's disease.
- Iioglobinuria.
- Channelopathies.
- Hereditary myopathies.
- Muscular dystrophies.
- Diseases of peripheral nerves.
- Diseases of the neuromuscular junction.
- Myasthenia.
- Lambert-Eaton syndrome.
- Botulism.
- Tick paralysis.
- Motor neuron diseases.
- Amyotrophic lateral sclerosis.
- Lower motor neuron diseases.
- Spinal muscular atrophy.
- Monomelic amyotrophic lateral sclerosis.
- Kennedy's disease.
- Upper motor neuron diseases.
- Hereditary spastic paraparesis.
- Primary lateral sclerosis.
- Diseases of the neuromuscular junction.
SYMPTOMS OF NEUROMUSCULAR DISEASES
The main symptom of neuromuscular diseases is muscle weakness. The clinical picture depends on the affected area (shoulder girdle, hips, pelvis, lower extremities, facial muscles, respiratory muscles). Depending on the form of the disease, muscle weakness and increased fatigue during physical activity develop, muscle atrophy / pseudohypertrophy, fasciculations appear, tendon reflexes are inhibited , gait is disturbed, special motor techniques appear when getting up from a lying or sitting position. Neuromuscular diseases occur in stages. A neurologist will help determine the stage of development of pathological processes using medical diagnostics.
Genetic panel "Neuromuscular diseases"
The panel combines diseases characterized not only by dysfunction of skeletal muscles, but also by pathology of neurons and pathways. The panel also includes a group of neurodegenerative and metabolic diseases that have similar clinical manifestations, which makes differential search easier. The prevalence of neuromuscular diseases ranges from 2.4-33.8 per 100,000 people, and the incidence varies according to various sources from 1.16 to 19 per million people per year.
The key symptoms characteristic of diseases from this group are muscle weakness, atrophy, dystonia, myotonia, contracture formation, and fasciculations.
The panel includes 391 genes responsible for the occurrence of neuromuscular diseases: isolated and syndromic motor-sensory and sensory-autonomic neuropathies, congenital structural myopathies and muscular dystrophies, metabolic myopathies, spinal muscular atrophies, myasthenia, amyotrophic lateral sclerosis, myotonia and periodic paralysis, as well as a number of genes associated with diseases with similar clinical manifestations.
Genes studied: AARS, ABCC9, ABHD12, ABHD5, ACAD9, ACADM, ACADS, ACADVL, ACTA1, ACTC1, ACTN2, ACVR1, ADCY6, AGL, AGRN, AIFM1, AKAP9, ALDOA, ALG13, ALG14, ALG2, ALS2, AMPD1, ANG , ANK2, ANO5, ARHGEF10, ASAH1, ATL1, ATL3, ATP2A1, ATP2A2, ATP7A, ATXN2, B3GALNT2, B4GAT1, BAG3, BICD2, BIN1, BMPR2, BSCL2, C10orf2, C12orf65, C9orf72, CACNA1C, CACNA1D, CACNA 1S, CACNB2, CALR3 , CAPN3, CASQ1, CASQ2, CAV3, CCDC78, CCT5, CFL2, CHAT, CHCHD10, CHKB, CHMP2B, CHRNA1, CHRNB1, CHRND, CHRNE, CHRNG, CHST14, CLCN1, CNTN1, CNTNAP1, COL12A1, COL4A1, COL6A1, COL6A2, COL6A3 , COLQ, COX6A1, CPT2, CRYAB, CSRP3, CTDP1, DAG1, DAO, DARS, DCAF8, DCTN1, DES, DHTKD1, DMD, DNA2, DNAJB2, DNAJB6, DNAJC3, DNM2, DNMT1, DOK7, DPAGT1, DPM2, DPM3, DPP6 , DSC2, DSG2, DSP, DST, DTNA, DYNC1H1, DYSF, ECEL1, EGR2, EMD, ENO3, ERBB3, ERBB4, ERCC3, ERCC4, ERCC5, ERCC6, ERCC8, ETFA, ETFB, ETFDH, EXOSC3, EXOSC8, EYA4, FAM134B , FBLN5, FBN1, FBN2, FBXO38, FGD4, FHL1, FIG4, FKBP10, FKBP14, FKRP, FKTN, FLNC, FUS, FXN, G6PC, GAA, GAN, GARS, GBE1, GDAP1, GFPT1, GJA1, GJA5, GJB1, GLA , GLE1, GMPPB, GNB4, GNE, GPD1L, GRN, GYG1, GYS1, GYS2, HADH, HADHA, HADHB, HARS, HCN4, HEXA, HINT1, HK1, HNRNPA1, HNRNPA2B1, HNRNPDL, HOXD10, HSPB1, HSPB3, HSPB8, IGHMBP2 , IKBKAP, INF2, ISCU, ISPD, ITGA7, JPH1, JPH2, JUP, KARS, KBTBD13, KCNA5, KCND3, KCNE1, KCNE2, KCNE3, KCNH2, KCNJ2, KCNJ5, KCNQ1, KIF1A, KIF1B, KIF5A, KLHL40, KLHL41, LAMA2 , LAMA4, LAMB2, LAMP2, LARGE, LDB3, LDHA, LITAF, LMNA, LMOD3, LPIN1, LRP4, LRSAM1, MAMLD1, MARS, MATR3, MED25, MEGF10, MFN2, MPZ, MSTN, MTM1, MTMR14, MTMR2, MUSK, MYBPC1 , MYBPC3, MYF6, MYH14, MYH2, MYH3, MYH6, MYH7, MYH8, MYL2, MYL3, MYLK2, MYOT, MYOZ2, MYPN, NALCN, NDRG1, NEB, NEFH, NEFL, NEXN, NGF, NPPA, NTRK1, OPA1, OPA3 , OPTN, ORAI1, PABPN1, PDHA1, PDK3, PFKM, PFN1, PGAM2, PGK1, PGM1, PHKA1, PHKA2, PHKB, PHKG2, PIEZO2, PIP5K1C, PKP2, PLEC, PLEKHG5, PLN, PLOD2, PMP22, PNPLA2, POLG, POLG 2 , POMGNT1, POMGNT2, POMK, POMT1, POMT2, PRDM12, PRKAG2, PRPH2, PRPS1, PRX, PSEN1, PSEN2, PTRF, PUS1, PYGL, PYGM, RAB7A, RAPSN, RAX2, RBCK1, RBM20, REEP1, RNF170, RRM2B, RYR1 , RYR2, SBF1, SBF2, SCN10A, SCN11A, SCN1B, SCN3B, SCN4A, SCN4B, SCN5A, SCN9A, SCO2, SEPN1, SEPT9, SETX, SGCA, SGCB, SGCD, SGCE, SGCG, SH3TC2, SIGMAR1, SIL1, SLC12A6, SLC16A1 T AZ , TBK1, TCAP, TDP1, TFG, TGFB3, TIA1, TK2, TMEM43, TMEM5, TMPO, TNNC1, TNNI2, TNNI3, TNNT1, TNNT2, TNNT3, TNPO3, TPM1, TPM2, TPM3, TRAPPC11, TRDN, TRIM2, TRIM32, TRPA1 , TRPM4, TRPV4, TTN, TTR, TUBA4A, TYMP, UBA1, UBQLN2, VAPB, VCL, VCP, VMA21, VRK1, WNK1, YARS, YARS2, ZBTB42, ZC4H2
Material for research: Venous blood with EDTA 2 ml.
Preparation for analysis: no
DIAGNOSTICS
The diagnostic task is to establish the level of damage to the neuromuscular system, establish the cause and determine whether there is a specific treatment.
- Electroneuromyography and electromyography. Diagnostic methods help determine primary and secondary myopathy. Also assess the degree of damage to the spinal cord and peripheral nerves.
- Laboratory tests. A clinical and biochemical blood test is required to determine the level of electrolytes, protein, lactate, CPK, ALT, AST, myoglobin and thyroid hormones.
- Muscle biopsy with pathomorphological examination of muscle tissue. The diagnostic results help to establish an accurate diagnosis (Duchenne, Becker muscular dystrophy), which is important for selecting the correct therapy.
- Molecular genetic diagnostics is the most informative diagnostic method, which is prescribed for neuromuscular diseases.
- Magnetic resonance imaging of the brain and cervical spine.
- An electrocardiogram (ECG) evaluates heart rhythm.
- ECHO CG reveals hypertrophic, dilated cardiomyopathy.
Basic methods for diagnosing hereditary lesions of the nervous system
Treatment of hereditary diseases of the nervous system abroad is carried out after a thorough examination of the patient and consultation with a geneticist.
Traditional research methods include:
- physical examination and determination of the level of tendon-muscular reflexes;
- radiography;
- CT scan;
- Magnetic resonance imaging;
- electron positron tomography.
Medical genetic examination includes the following methods:
- genealogy. Finding out information about the presence of the disease in the patient’s family members makes it possible to establish the hereditary nature of the pathology;
- cytogenetics. The technique detects chromosomal mutations;
- biochemistry. This diagnostic method clarifies the state of metabolic processes in the patient’s body;
- antenatal diagnosis is a method of identifying genetic mutations of the fetus in the womb.
TREATMENT OF NEUROMUSCULAR DISEASES
As for treatment, there is no specific therapy. The therapeutic approach is based on creating the prerequisites for successful rehabilitation and providing high quality general and specialized care.
- Drug therapy. The goal is to compensate for the energy deficiency of muscle tissue, improve tissue metabolism and peripheral circulation. Myotropic drugs and anabolic steroids are used. In the case of Duchenne muscular dystrophy, glucocorticosteroids are used. In the case of myasthenia gravis, anticholinesterase drugs are used. For secondary damage and/or dysfunction of the central nervous system, courses of neuroprotective and neurotrophic therapy are carried out. Drug therapy for bulbar and pseudobulbar disorders.
- Physiotherapy. The goal is to correct metabolic disorders, improve neuromuscular conduction, normalize muscle tone, and prevent the development of contractures.
- Physiotherapy. The goal is to prevent the development and correction of contractures of the limbs, maintain motor activity, improve muscle tone, delay the development of atrophies, and prevent complications caused by inactivity. Teaching the patient how to use assisted sitting and standing devices.
- Orthopedic correction.
- Early detection of swallowing disorders (dysphagia) and the possibility of drug correction (together with ENT doctors, based on the results of nasopharyngoscopy - the functional state of the epiglottis, the presence of regurgitation, and in older children + analysis of the results of an X-ray contrast study of the act of swallowing).
- Neurological assessment of respiratory function (ENMG analysis of the phrenic nerves + ultrasound of the diaphragm, analysis of respiratory function, pulse oximetry and capnometry, mechanics and type of breathing, ECHO data, ECG with a cardiologist’s conclusion).
Neurological examination of patients for respiratory failure makes it possible to clarify its causes, reversibility of disorders and the degree of their compensation. In the case of an established dependence on mechanical ventilation, work in a team of doctors to create a multifunctional therapeutic program that is aimed at improving physical condition and restoring normal life functions. choice of treatment methods and their order (medication and non-medication, including management of respiratory support parameters, breathing exercises, physical therapy, physiotherapeutic techniques, psychological assistance, etc.).
Congenital myopathies in children
Neuromuscular diseases can be hereditary, autoimmune and metochondrial.
1. Thomsen's myotonia is inherited and manifests itself in early childhood. The first sign is a swallowing disorder (slow swallowing, frequent vomiting), which occurs due to high tone of the pharyngeal muscles. Over time, the inability to unclench fingers clenched into a fist and difficulty in starting to walk occurs. Only muscle strength, due to the tone of skeletal, and not smooth muscles, does not suffer.
2. In muscular dystrophy, the muscle fibers themselves are damaged. The following symptoms are typical for muscle weakness in a child:
- muscle weakness;
- decreased muscle tone;
- children's lag in motor development;
- atrophy (“drying”) of muscles or a false increase in muscle volume due to their replacement with adipose tissue;
- skeletal deformities.
3. In case of amyotrophy, the nerve fibers of the spinal cord or the nerves themselves are affected. Already from birth you can notice in a child:
- lethargy (frog pose);
- slowdown in motor development (the child begins to hold his head up late, sit up, walk);
- "duck" gait;
- “wing-shaped” shoulder blades;
- “wasp” waist;
- increase in muscle volume (“athlete’s body”).
Diagnosis and treatment of muscle diseases
Therapy for neuromuscular diseases depends on proper diagnosis. It can be medication, physiotherapy, vitamin therapy, exercise therapy, etc. With the development of joint contractures and spinal deformities, orthopedic correction is used.
An integrated approach to the treatment of children with muscle weakness slows down the progression of the disease.
To treat neuromuscular diseases, drugs that improve the metabolism of nervous muscle tissue, anabolic steroids, drugs that improve neuromuscular conduction, etc. are used. Drug therapy is prescribed by the attending physician.
Prevention of muscle disease in the unborn child is carried out during medical and genetic counseling of parents at the stages of family planning. Thus, the risks of developing hereditary diseases, including muscle pathologies, are assessed.