Types of lymphomas
There are two main groups of the disease – Hodgkin lymphoma and non-Hodgkin lymphoma. They develop from different types of cells, differ in their course and respond differently to therapy.
Hodgkin's lymphoma (HLH) is lymphogranulomatosis, malignant granuloma. Characterized by damage to B-lymphocytes. It has an aggressive course, but responds well to treatment. Source: I.I. Yakovtsova, V.D. Sadchikov, V.M. Sadchikova, O.V. Dolgaya, S.V. Danilyuk, A.E. Oleynik Hodgkin's lymphoma: evolution of clinical classifications // Bulletin of problems of biology and medicine, 2013, No. 3, v. 2 (103), pp. 62-69
Non-Hodgkin's lymphomas (NHL) affect not only B-, but also T-lymphocytes. A total of 30 subtypes have been identified. Most of them are less aggressive, but also more difficult to treat.
Classification of non-Hodgkin's lymphomas in accordance with the 4th edition of WHO 2008:
- B-lymphoblastic NHL;
- heavy chain disease;
- B-cell prolymphocytic leukemia;
- hairy cell leukemia;
- diffuse large B-cell NHL;
- Burkitt's leukemia;
- NHL from mantle zone cells;
- lymphoplasmacytic NHL;
- mediastinal diffuse large B-cell NHL;
- nodal marginal zone B-cell NHL;
- primary exudative NHL;
- plasma cell plasmacytoma/myeloma;
- splenic marginal zone NHL;
- follicular NHL;
- chronic lymphocytic leukemia;
- extranodal marginal zone B-cell NHL;
- T-lymphoblastic NHL;
- aggressive NK cell leukemia;
- anaplastic large cell NHL with primary skin lesions;
- anaplastic large cell NHL with primary systemic involvement;
- angioimmunoblastic T-cell NHL;
- hepatolienal T-cell NHL;
- Sézary's mycosis fungoides;
- unspecified peripheral T-cell NHL;
- T-cell panniculitis-like NHL of the subcutaneous tissue;
- T-cell leukemia;
- T-cell leukemia of large granular lymphocytes;
- T-cell prolymphocytic leukemia;
- extranodal NK/T-cell lymphoma of the nasal type;
- enteropathic T-cell NHL.
The most common lymphomas in clinical practice are: Hodgkin, follicular and diffuse large B-cell. Source: G.S. Tumyan Non-Hodgkin lymphoma // Clinical oncohematology, 2015, 8(4), pp.455-470
According to the nature of the lesion and pathogenesis, all lymphomas are divided into 3 main groups:
- aggressive – they are characterized by rapid development with pronounced symptoms;
- extranodal - the primary lesion is formed not in the lymph nodes, but immediately in the internal organs;
- indolent - distinguished by their slow and favorable course; may not require therapy; sometimes it is enough to see a doctor regularly.
For each type of lymphoma there is a special treatment regimen.
Classification of non-Hodgkin's lymphomas
The most commonly used is the European-American classification developed within the World Health Organization (WHO).
According to this classification, NHLs are divided depending on their cellular identity.
Diffuse large B-cell lymphoma accounts for 31% of the total number of lymphomas. This lymphoma occurs most often after age 60 and grows rapidly. At the same time, 40-50% of patients can be completely cured.
Follicular lymphoma , which accounts for 22% of total NHL. This type of lymphoma is usually diagnosed around age 60 and is characterized by slow growth. Long-term (5-year) survival of patients ranges from 60-70%. Over time, follicular lymphoma can develop into a fast-growing diffuse lymphoma.
Chronic lymphocytic leukemia/small cell lymphocytic lymphoma. These related diseases account for 7% of the total number of lymphomas. They are characterized by slow growth, but are difficult to treat. However, patients with these diseases can live for 10 years. Sometimes it is possible to transform them into fast-growing lymphomas.
Mantle cell lymphoma (6%) most often affects men around 63 years of age. Although this type of lymphoma does not grow very quickly, only 20% of patients live for 5 years.
Extranodal marginal zone B-cell lymphomas—MALT lymphomas (8%). The average age of patients is about 60 years. Often found in the stomach, it is characterized by slow local growth. It can be cured well in the early stages.
Nodal marginal zone B-cell lymphoma (2%). Characterized by slow growth. Many patients with early stages of the disease can be completely cured.
Splenic marginal zone B-cell lymphoma occurs in elderly patients, most often males. Often, treatment is not prescribed until severe symptoms appear as a result of an enlarged spleen.
Primary mediastinal B-cell lymphoma (2%) occurs in the mediastinum mainly in women aged 30-40 years and is characterized by rapid growth. 50% of patients can be cured.
Burkitt's lymphoma and Burkitt-like lymphoma (2%) occurs in 90% of cases in men aged about 30 years. Characterized by rapid growth. With intensive chemotherapy, 50% of patients can be completely cured.
Lymphoplasmacytic lymphoma (Waldenström's macroglobulinemia) accounts for 1% of the total number of NHLs. The disease is characterized by a slow progression, but it cannot be completely cured. However, most patients live more than 5 years.
Hairy cell leukemia is a very rare disease and is detected in older people. Characterized by slow growth. Some patients do not need treatment.
Primary central nervous system (CNS) lymphoma can affect both the brain and spinal cord. Previously, this tumor was considered very rare, but now it is detected more often in patients with AIDS. 30% of patients live 5 or more years.
T-lymphoblastic lymphoma/progenitor cell leukemia (2%). This disease can be considered lymphoma or leukemia. The difference depends on the number of tumor cells in the bone marrow. If less than 25% of tumor cells are detected, a diagnosis of lymphoma is made, and more than 25% - leukemia.
75% of patients are men, and the remaining 25% are women. The average age of patients is 25 years. If the bone marrow is not affected, then the probability of cure is high, and if it is involved in the process, the probability of cure does not exceed 20%.
Peripheral T-cell lymphomas (7%) are divided into several types:
Cutaneous T-cell lymphoma (mycosis fungoides, Sezary syndrome) accounts for less than 1% of all lymphomas and is detected at the age of 50-60 years. The 5-year survival rate of patients ranges from 5 to 58%, depending on the rate of tumor growth.
Angioimmunoblastic T-cell lymphoma is characterized by rapid growth and a poor prognosis.
Extranodal T-cell lymphoma of natural killer cells , nasal type, occurs in all age groups. The outcome of the disease depends on the degree of spread of the tumor process.
T-cell lymphoma with enteropathy occurs in people who are sensitive to gluten, a protein in wheat flour. The prognosis (outcome) of the disease is unfavorable.
Subcutaneous T-cell panniculitis-like lymphoma grows slowly at first but can become a fast-growing tumor over time. Chemotherapy is only partially effective.
Anaplastic large cell lymphoma, T/0-cell (2%) occurs more often in young people. Chemotherapy can cure many patients.
Stages of lymphomas
Depending on the extent of the tumor, the stage of the pathological process is determined. In accordance with the international Ann Arbor classification, there are 4 stages of the disease:
- At stage 1, one group of lymph nodes may be involved in the lymphoma process.
- On the 2nd, the involvement of two or more groups on one side of the diaphragm is allowed.
- At stage 3, the lymph nodes on both sides of the diaphragm are affected.
- At the 4th stage, internal organs are involved in the process - the brain, heart, liver, spleen, stomach, intestines.
Each stage is additionally marked with titers A and B. Titer A indicates the absence of key symptoms - fever, severe night sweats and sudden weight loss. Titer B indicates that such manifestations exist.
Lymphoma
Typically, the first symptom of lymphoma is a significant increase in the size of the lymph nodes in the neck, armpits, or groin. Moreover, unlike infectious diseases, enlarged lymph nodes are painless, their size does not decrease over time and when treated with antibiotics. Sometimes, due to pressure from the enlarged liver, spleen and lymph nodes, there is a feeling of fullness in the abdomen, difficulty breathing, bursting pain in the lower back, a feeling of pressure in the face or neck
Other symptoms encountered with lymphoma are:
- Weakness
- Increased body temperature
- Sweating
- Weight loss
- Digestive disorders
Types of lymphomas
The term non-Hodgkin's lymphoma refers to a fairly large group of lymphomas that are not Hodgkin's disease (lymphogranulomatosis). The decision whether a lymphoma belongs to the group of non-Hodgkin's lymphomas or to Hodgkin's disease is made after a histological examination of a sample of biopsied tissue. If, during microscopic examination, Berezovsky-Sternberg-Reed cells specific for Hodgkin's disease are found, then a diagnosis of Hodgkin's disease is made. If these specific cells are not found, then the lymphoma is classified as non-Hodgkin's.
Non-Hodgkin's lymphomas have many subtypes, which differ in histological appearance, clinical manifestations and approaches to their treatment. Some types of lymphomas have a slow and favorable course, and sometimes do not require special treatment for a long time. Such lymphomas are called indolent . A number of other lymphomas, on the contrary, are characterized by rapid progression, a large number of symptoms and require immediate treatment. Such lymphomas are called aggressive . There are lymphomas with intermediate characteristics. Most often, abnormal growth of lymphocytes begins in the lymph nodes, and the classic version of lymphoma develops, accompanied by enlarged lymph nodes. However, there are lymphomas in which the lymph nodes do not enlarge, because the disease primarily occurs not in the lymph node, but in various organs: spleen, stomach, intestines, lungs, brain. Such lymphomas are called extranodal .
For a long time, in many countries there were different classifications, including different names and terms for the same type of non-Hodgkin lymphoma, which created great difficulties for both doctors and patients. In 2001, the international community developed unified approaches to the classification of lymphomas, and a single, so-called World Health Organization (WHO) classification was adopted, which is used today in most countries of the world.
We present the WHO classification in full. If desired, everyone can familiarize themselves with it as much as they consider necessary.
Lymphoma stages
Determining the stage of lymphoma helps to understand the extent of the disease. This is important information for making the right decision regarding your treatment program. Approaches to the treatment of early (local) stages and advanced stages of lymphomas usually differ. When choosing a treatment program, not only the stage is taken into account, but also many other factors: the type of lymphoma, the results of additional studies (cytogenetic, immunological, molecular, etc.), the patient’s condition, his age, concomitant diseases, etc. However, information about the stage of the disease is extremely important for developing an effective treatment program.
In accordance with the generally accepted international classification (it is called the Ann Arbor classification after the name of the city in the USA where it was adopted), there are 4 stages of the disease: I, II, III and IV. The letters A or B are usually added to the stage number. These letters indicate the presence or absence of 3 important symptoms that can occur in patients with lymphoma: fever, severe night sweats and weight loss. If the letter A is used, this means that the above symptoms are absent, if the letter B is used, this indicates that the patient has the above symptoms.
The classification identifies four stages of the disease, which can be conditionally designated as local (local, limited) - stages I and II and widespread - stages III and IV.
- Stage I - involvement of one area of lymph nodes in the lymphoma process is allowed
- Stage II - two or more areas of lymph nodes on one side of the diaphragm are allowed to be involved in the process (the diaphragm is a muscular layer that separates the chest and abdominal cavity).
- Stage III - damage to the lymph nodes on both sides of the diaphragm is allowed.
- Stage IV - the disease spreads in addition to the lymph nodes to the internal organs: heart, liver, kidneys, intestines, bone marrow, etc.
World Health Organization classification of non-Hodgkin's lymphomas
B-cell tumors from B-lymphocyte precursors:
- B-lymphoblastic lymphoma/progenitor cell leukemia (B-cell acute lymphoblastic leukemia from progenitor cells).
- B-cell tumors from peripheral (mature) B-lymphocytes:
- B-cell chronic lymphocytic leukemia/small lymphocyte lymphoma (lymphocytic lymphoma)
- B-cell prolymphocytic leukemia
- Lymphoplasmacytic lymphoma
- Splenic marginal zone lymphoma (+/- villous lymphocytes)
- Hairy cell leukemia
- Plasma cell myeloma/plasmacytoma
- Extranodal marginal zone B-cell lymphoma MALT type
- Nodal marginal zone B-cell lymphoma (+/- monocytoid B lymphocytes)
- Follicular lymphoma
- Mantle cell lymphoma
- Diffuse large B cell lymphoma
- Mediastinal diffuse large B-cell lymphoma
- Primary exudative lymphoma
- Burkitt's lymphoma/leukemia
T- and NK-cell tumors from T-lymphocyte precursors
- T-lymphoblastic lymphoma/progenitor cell leukemia (T-cell acute lymphoblastic leukemia from progenitor cells)
T-cell lymphomas from peripheral (mature) T-lymphocytes:
- T-cell prolymphocytic leukemia
- T-cell leukemia of large granular lymphocytes
- Aggressive NK cell leukemia
- Adult T-cell lymphoma/leukemia (HTLV1+)
- Extranodal NK/T-cell lymphoma, nasal type
- T-cell lymphoma associated with enteropathy
- Hepatolienal T-cell lymphoma
- T-cell panniculitis-like lymphoma of subcutaneous tissue
- Mycosis fungoides/Sézary syndrome
- Anaplastic large cell lymphoma, T/0 cell, with primary skin involvement
- Peripheral T-cell lymphoma, unspecified
- Angioimmunoblastic T-cell lymphoma
- Anaplastic large cell lymphoma, T/0 cell, with primary systemic involvement
The given forms of non-Hodgkin's lymphomas are also divided depending on the characteristics of their clinical course into aggressive and indolent.
Causes of lymphomas
A single causative factor for the development of the disease has not been identified. At the moment, scientists believe that the pathological process is triggered by a complex of reasons. These include:
- hereditary predisposition;
- regular contact with toxins and carcinogens;
- herpes virus, hepatitis, Helicobacter pylori and other infectious diseases;
- autoimmune and immunodeficiency conditions;
- recurring pneumonia;
- immunosuppressive therapy after kidney transplantation, stem cell transplantation, etc.;
- surgery to insert breast implants (presumably).
Symptoms
In addition to the main symptoms - fever, severe night sweats and sudden weight loss - the pathology is characterized by:
- weakness and increased fatigue;
- temperature increase;
- weight loss;
- enlarged lymph nodes (often, but not always; they are painless and do not shrink as a result of treatment with antibiotics, as with infectious diseases).
Sometimes itchy skin is possible. When a chest tumor is affected, difficulty breathing, shortness of breath and cough are possible. When the tumor is localized in the abdominal cavity, indigestion, nausea, vomiting, and bursting pain in the abdomen and lower back are observed. When the bone marrow is damaged, patients complain of pain in the bones. If the pathology involves facial and cranial structures, there are complaints of headaches and bursting pain in the face and neck.
Lymphomas (lymphogranulomatosis and non-Hodgkin's lymphomas)
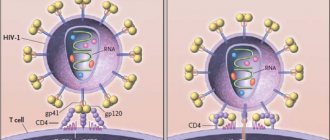
HIV
Gastritis
Ulcer
Hepatitis
32014 November 23
IMPORTANT!
The information in this section cannot be used for self-diagnosis and self-treatment.
In case of pain or other exacerbation of the disease, diagnostic tests should be prescribed only by the attending physician. To make a diagnosis and properly prescribe treatment, you should contact your doctor. Lymphomas: causes, symptoms, diagnosis and treatment methods.
Definition
Lymphomas are a group of malignant tumor diseases of the lymphatic tissue, which under normal conditions is responsible for immunity. One of the first clinical symptoms of lymphoma is enlargement of lymph nodes in different locations.
Lymphomas, like other malignant tumors, have a tendency to metastasize, that is, the migration of tumor cells through the blood and lymph, as well as through contact into intact (healthy) tissues with subsequent reproduction in them.
Almost all types of lymphogranulomatosis, or Hodgkin's lymphoma, and about 65% of non-Hodgkin's lymphomas manifest as painless enlargement of the lymph nodes - 2 cm or more. However, the diagnosis of a particular type of lymphoma is established solely on the basis of a morphological examination of biopsy material taken from the tumor.
The incidence of Hodgkin's lymphoma in Russia is about 2 cases per 100 thousand population per year, and non-Hodgkin lymphoma is 5–7 cases per 100 thousand.
Causes of lymphomas
There are several possible causes for the development of lymphomas. It is important to understand that the basis for the development of any malignant disease, including lymphomas, is a dysfunction of cells.
The ability for uncontrolled tumor growth occurs when the natural process of cell division is disrupted: normally, the cell divides a limited number of times, matures, performs a certain function, and then ends its life.
Malignant cells are characterized by disruption of the processes of maturation and differentiation (the process during which the cell acquires specific characteristics and the ability to perform certain functions). Cells acquire new functions - they begin to produce proteins and toxins, and the ability to “escape immune surveillance” appears, as a result of which the process of natural cell death (apoptosis) changes.
Some viruses can directly affect the DNA of lymphocytes and contribute to their transformation into malignant cells.
For example, infection with Epstein–Barr virus (EBV) is an important risk factor for the development of lymphomas.
Lymphocytes are divided into two subtypes: T and B cells (T and B lymphocytes). Infection with human T-cell lymphotropic virus (HTLV-1) increases a patient's risk of developing certain types of T-cell lymphoma. The virus is transmitted sexually and through blood, as well as from mother to child through breast milk.
Viruses that weaken immunosurveillance are indirectly responsible for the development of certain types of lymphomas.
Thus, the human immunodeficiency virus (HIV) reduces the population of lymphocytes, while the control of mutant cells and herpes viruses type 8 and Epstein-Barr decreases with the formation of lymphomas.
Some infections can cause the development of lymphoma due to the constant activation of the immune system. Chronic infections produce a huge number of lymphocytes, which increases the likelihood of mutations during cell division and leads to the risk of lymphoma. Similar infections include Helicobacter pylori
(often found in chronic gastritis and peptic ulcers of the stomach and duodenum),
Chlamydophila psittaci
(risk of developing lymphoma in the tissues of the eye), hepatitis B and C viruses with prolonged infection.
Non-infectious risk factors for the development of lymphomas include:
- Exposure to chemicals. Numerous studies have shown that exposure to herbicides, insecticides, and benzene is associated with an increased risk of developing lymphomas.
- The presence of autoimmune diseases (rheumatoid arthritis, systemic lupus erythematosus, etc.) is a significant risk factor for the development of lymphomas.
- Radiation exposure has a great influence on the rate of cell mutations and their malignancy.
- Genetic factors. Having a close relative with lymphoma greatly increases your risk.
- Congenital immune deficiency in certain diseases.
- Age. Some types of lymphoma develop in children and adolescents, while others, on the contrary, develop in people over 60 years of age.
- Breast implants can rarely lead to the development of a type of large cell lymphoma of the breast.
Classification of lymphomas
There are two main types of lymphomas: Hodgkin's lymphoma, or lymphogranulomatosis, and non-Hodgkin's lymphomas.
Hodgkin lymphoma is characterized by the presence of specific Reed-Berezovsky-Sternberg cells in the affected lymph nodes, spleen, liver or bone marrow.
Enlarged cervical lymph nodes in a patient with Hodgkin lymphoma
The group of non-Hodgkin's lymphomas includes:
- follicular lymphoma;
- marginal zone lymphoma;
- diffuse large B-cell lymphoma;
- mantle cell lymphoma;
- Burkitt's lymphoma;
- primary lymphoma of the central nervous system;
- nodal T-cell lymphomas;
- primary cutaneous lymphomas;
- non-Hodgkin's lymphomas in patients infected with HIV;
- non-Hodgkin's lymphoma in patients infected with hepatitis B and C viruses.
Symptoms of lymphomas
The earliest symptom is enlarged lymph nodes against the background of complete well-being. Enlarged lymph nodes are painless.
Various clinical manifestations depend on the location of the tumor: if the tumor grows in the lymph nodes of the chest, compression of the airways and the appearance of hoarseness, difficulty swallowing, difficulty breathing, and obsessive cough are possible.
When lymphoma is located in the mediastinum, compression syndrome of the superior vena cava appears: headaches, swelling and dilation of the veins of the face and neck occur.
In some cases, only general symptoms are present: loss of appetite, weight loss, increased body temperature, night sweats, weakness, and sometimes itchy skin and pain in enlarged lymph nodes.
Against the background of a decrease in immunity, infectious diseases can occur - the chickenpox virus is often activated, manifested by herpes zoster.
Cases of damage to the abdominal organs (manifested by an increase in the volume of the abdomen due to tumor growth and fluid accumulation, the appearance of pain, jaundice, nausea and vomiting) and bone marrow (pain in the bones, back, frequent fractures, pallor, increased bleeding) have been described.
Diagnosis of lymphomas
The diagnosis of a particular type of lymphoma is established solely on the basis of a morphological examination of biopsy material (a piece or a whole lymph node obtained during a minor operation) taken from the tumor (histological, cytogenetic and molecular genetic research methods). The doctor will prescribe additional tests to diagnose the stage of the disease and its complications. The list of studies depends on the presumed location of the tumor and may be changed.
- Clinical blood test.
Diagnosis of lymphomas
The diagnosis is made based on the results of a microscopic examination of a biopsy - a sample of lymphoid tissue. Based on the results of a differential biopsy, the type of tumor is determined.
To identify tumors in different parts of the body, radiation diagnostic methods are used: radiography, scintigraphy, magnetic resonance, positron emission and computed tomography. If it is necessary to clarify some features of the pathological process, laboratory blood tests are prescribed - immunoenzyme typing using flow cytometry, molecular genetic and cytogenetic studies. Source: Wang HW, Balakrishna JP, Pittaluga S, Jaffe ES Diagnosis of Hodgkin lymphoma in the modern era // Br J Haematol. 2021 Jan;184(1):45-59. doi: 10.1111/bjh.15614. Epub 2021 Nov 8
Treatment methods for lymphoma at Medscan
The medical center treats lymphoma using gentle chemotherapy and the latest radiation exposure. If necessary, a course of immunotherapy is prescribed on an individual basis.
The clinic uses drugs developed by Medscan. Treatment of lymphoma with antitumor drugs is carried out strictly according to the international ESMO or NCCN protocols and has a high level of positive results. For intravenous administration of drugs, infusion pumps are used to control the dosage of the drug.
A favorable prognosis for a malignant form of pathology depends on a number of factors. Has the meaning:
- Localization, type and size of the tumor. Neoplasms in the early stages are easier to cure.
- Forms of the disease. Aggressive cancer manifests itself with a clear clinical picture, which indicates damage to internal organs.
- Lymphoma stage. The chances of recovery in advanced stages of pathology are minimal.
After treatment, the clinic’s specialists provide the patient with the necessary information about the cancer disease. The signs of relapse and subsequent routine examinations are explained. After completing treatment for non-Hodgkin's lymphoma, the patient is required to undergo systematic monitoring by the attending physician.
Improvements in diagnostic and therapeutic methods have made it possible to achieve optimal results in most patients. Prognostic factors for lymphomas are used to guide therapy rather than to estimate survival.
Treatment methods
The most common treatments for lymphomas are:
- radiation therapy;
- chemotherapy;
- radiotherapy;
- biological therapy;
- stem cell transplantation;
- surgical intervention.
They are used both as separate courses and in combination. The choice of treatment regimen depends on the type of tumor and the general condition of the patient.
Treatment tactics
Indolent lymphomas may not require treatment, but only observation by an oncohematologist. Therapy is indicated at the first signs of progression of the pathological process. For localized tumors, radiotherapeutic irradiation of the affected structures is sufficient. For generalized forms, chemotherapy is indicated.
In case of an aggressive course of the disease, one of the most effective treatment regimens is chemotherapy according to the CHOP protocol in combination with immunotherapeutic drugs from the group of monoclonal antibodies. For highly aggressive types of tumors, high-dose chemotherapy in combination with hematopoietic stem cell transplantation may be prescribed.
Treatment of certain types of lymphomas
The main method of treatment for Hodgkin lymphoma LGM is chemotherapy. Antitumor cytotoxins are prescribed in different dosage forms. Chemotherapy is cyclical in nature - drug courses alternate with periods of rehabilitation. Source: Sermer D, Pasqualucci L, Wendel HG, Melnick A, Younes A Emerging epigenetic-modulating therapies in lymphoma // Nat Rev Clin Oncol. 2019 Aug;16(8):494-507.doi: 10.1038/s41571-019-0190-8
Radiotherapy - high-power radiation - as an independent treatment for LM may be justified in some cases - when one, maximum two groups of lymph nodes are involved in the process. More often it is prescribed in combination with chemotherapy. In the later stages of the disease, the method is indicated as palliative treatment.
Biological drugs - monoclonal antibodies - are used in the treatment of lymphoma to activate the immune system. Radiation therapy is carried out regionally, in the area of the lymph nodes involved in the oncological process.
In some cases, removal of the spleen is justified in the treatment of LGM. If enlarged lymph nodes are compressing neighboring organs, their excision may be indicated.
In case of relapses of the disease, as well as in order to destroy cancer cells that are not affected by standard doses of radiation and chemotherapy, high therapeutic doses are prescribed, which destroy bone marrow tissue along with the tumor. After such a course, organ transplantation is indicated. Your own or donor stem cells taken in advance form a new immune system.
A combination of radiation and chemotherapy also demonstrates good results in the treatment of NHL. In some cases, the innovative technique of lumbar puncture administration of antitumor antibodies is successfully used.
NHL with an aggressive course is difficult to treat. The most effective method to combat this disease is a bone marrow transplant.
What types of non-Hodgkin's lymphomas are there?
Today, scientists distinguish two types of non-Hodgkin lymphomas, which are associated with their origin:
- B-lymphocyte NHL. B cell precursors, mature cell and B cell proliferation of uncertain malignant potential;
- T lymphocytes and natural killer cells (NK lymphocytes) NHL. T cell precursors, extranodal mature T cells and NK cells, and nodal T and NK cells.
In 2021, the WHO revised the full classification of NHL to include more than 60 subtypes. It is considered the most accurate and informative, since everything is taken into account: genotypes, immunophenotypes and many other characteristics of the tumor.
https://pubmed.ncbi.nlm.nih.gov/26980727/
At the same time, NHL from B lymphocytes occurs in 85-90% of cases, and only 10-15% occurs in T lymphocytes and NK lymphocytes. ( https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(12)60605-9/fulltext )
Separately, it is worth highlighting the clinical classification of the course of the tumor.
- Indolent. Slow spread, affects bone marrow, liver and spleen. Most often, patients live a long time, sometimes even without treatment.
- Aggressive. A sharp manifestation, with a rapid deterioration in the general condition of the body, metastases are often observed. Without treatment, the patient can live up to several years, but they easily respond to generally accepted treatment principles.
- Highly aggressive. They are difficult to treat, the clinic appears immediately, it is difficult to treat. Without treatment, death occurs within a few months.
Additionally, NHL is conventionally divided according to the location of the tumor:
- NHL of the stomach or intestines;
- skin NHL;
- NHL of the brain;
- NHL of the chest.
The Lugano staging classification is used to help the doctor understand the extent of the cancer's spread.
First stage
The presence of one affected lymph node or one internal organ.
Second stage
Lymphoma was found in two or more groups of lymph nodes, but all of them were on one side of the diaphragm (bottom or top). Or a group of lymph nodes is located in the same location of a neighboring organ.
Third stage
NHL located above and below the diaphragm and in the spleen.
Fourth stage
Lymphomas in the lymph nodes and in the bone marrow\liver\lungs.
Forecasts
The prognosis for patients with lymphoma depends on the stage of the process, the age and condition of the patient, as well as on the results of therapy. With Hodgkin's lymphoma, young patients in the early stages usually make a full recovery. In 8 out of 10, stable remission is achieved. The five-year survival rate for stage 1 is 95%, for stage 4 – 65%.
For NHL of the spleen, lymph nodes and mucous membranes, the average five-year survival rate is about 70%. For NHL of the gastrointestinal tract, salivary glands, and eye orbits, the average five-year survival rate is about 60%. The prognosis for aggressive NHL of the mammary glands, ovaries, central nervous system and bones is less favorable - the five-year survival rate is on average less than 30%.
Diagnosis and treatment
If persistent symptoms of illness appear, it is recommended to consult a physician. The doctor will conduct an examination, study complaints and prescribe several diagnostic procedures;
- Ultrasound;
- blood and urine tests;
- MRI;
- CT;
- biopsy (sampling of a tissue fragment) of a lymph node;
- chest x-ray;
- if necessary, research using radioisotope methods.
Treatment is carried out in several directions, the main ones being chemotherapy and radiation therapy. In some cases, transplantation is used - for this they take their own stem cells or cells from a donor. Today, several treatment regimens have been developed. The use of a specific course of therapy depends on the stage of development of the disease, the type of lymphoma, age, condition of the patient and other factors.
Prognosis for recovery primarily depends on the type of aggressiveness. No less important is the stage at which oncological pathology is diagnosed. At the same time, even experienced specialists often cannot give an accurate forecast. But if treated in a timely manner, the chances of maintaining a good and long life are indeed much higher.
Clinical recommendations after lymphoma treatment and prevention
Avoid risk factors - intoxication and contact with carcinogens. Get vaccinated, and if you get an infectious disease, do not self-medicate.
At the first sign of lymphoma, consult your doctor. Get annual preventive medical examinations, eat right, and try to lead a healthy lifestyle.
Sources:
- I.I. Yakovtsova, V.D. Sadchikov, V.M. Sadchikova, O.V. Dolgaya, S.V. Danilyuk, A.E. Oleinik. Hodgkin's lymphoma: evolution of clinical classifications // Bulletin of problems in biology and medicine, 2013, No. 3, vol. 2 (103), pp. 62-69.
- G.S. Tumyan. Non-Hodgkin's lymphomas // Clinical oncohematology, 2015, 8(4), pp.455-470.
- Wang HW, Balakrishna JP, Pittaluga S, Jaffe E. Diagnosis of Hodgkin lymphoma in the modern era // Br J Haematol. 2019 Jan;184(1):45-59. doi: 10.1111/bjh.15614. Epub 2021 Nov 8.
- Sermer D, Pasqualucci L, Wendel HG, Melnick A, Younes A. Emerging epigenetic-modulating therapies in lymphoma // Nat Rev Clin Oncol. 2021 Aug;16(8):494-507.doi: 10.1038/s41571-019-0190-8.
The information in this article is provided for reference purposes and does not replace advice from a qualified professional. Don't self-medicate! At the first signs of illness, you should consult a doctor.
Lymphoma: what is it
Lymphoma is an oncological pathology that affects the lymphatic system. The development of the disease begins with rapid, uncontrolled cell division, which leads to the appearance of tumors. The pathology is dangerous and can lead to death. The success of treatment largely depends on how quickly the patient sees a doctor.
The exact causes of lymphoma, like many other cancers, are still unknown. In this case, we can name several provoking factors that can certainly contribute to the development of pathology:
- viral infections (mainly VID, some types of herpes, Epstein-Barr virus);
- bacterial infections;
- gender and age characteristics (more often in men over 55 years old);
- taking medications related to immunosuppressants;
- environmental impact (unfavorable environmental conditions, harmful working conditions);
- regular violation of the rules of a healthy lifestyle.