Raynaud's disease is one of the most mysterious diseases that affects about 5% of the world's population. It was first described in 1862 by the French physician, scientist and educator Maurice Raynaud ( Maurice Raynaud), who observed a girl suffering from sudden attacks of numbness in her limbs. Based on an analysis of five similar cases, the author concluded that these symptoms belonged to a new, previously unknown disease, and described in detail all its symptoms.
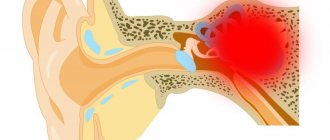
The disease manifests itself as sudden attacks of spasm in the small arteries of the arms and/or legs, and sometimes in other peripheral parts of the body - the tip of the nose and ears. As a result, blood ceases to flow in sufficient quantities to the cells of these parts of the body, leading to the development of so-called ischemia (bleeding). As a rule, this is preceded by hypothermia or severe stress. As the disease progresses, it can eventually lead to a serious complication - gangrene of the fingers.
Most often, the disease occurs in residents of cold climates and mainly affects middle-aged people (40-50 years old). Raynaud's syndrome occurs 4 times more often in women than in men.
1 General blood test
2 Diagnosis of Raynaud's syndrome
3 Diagnosis of Raynaud's syndrome
When talking about this disease, we mean two types of pathology: Raynaud's disease and Raynaud's syndrome .
Raynaud's disease is considered an independent disease with an unknown cause.
Raynaud's syndrome may be a manifestation of any other underlying diseases. When they talk about Raynaud's phenomenon, they most often (in most patients) mean Raynaud's syndrome. And only 15% of patients have an independent disease with the same name.
A mandatory sign of this disease is symmetrical damage to the limbs.
Causes of Raynaud's syndrome
Raynaud's syndrome can be a consequence of the following diseases and factors:
- various autoimmune connective tissue pathologies (systemic scleroderma, rheumatoid arthritis, systemic lupus erythematosus);
- inflammatory diseases of blood vessels - systemic vasculitis (granulomatosis or Wegener's disease, polyarteritis nodosa, drug-induced vasculitis, cryoglobulinemic vasculitis);
- blood diseases (thrombophlebitis, thrombocythemia, cryoglobulinemia, leukemia);
- diseases of the endocrine system (pathology of the adrenal glands and thyroid gland);
- hypothermia, stress, emotional overstrain;
- long-term use of medications that have a vasoconstrictor effect (migraine medications).
Raynaud's syndrome
Raynaud's syndrome (RS) is an episodic disorder of the peripheral circulation due to local arterial vasoconstriction (spasm) of the digital arteries and cutaneous vessels in response to exposure to cold or emotional stress. Clinically, the syndrome manifests itself as sharply defined changes in the color of the skin of the fingers. Increased vascular spasm is based on a defect in the central and local mechanisms of regulation of vasomotor reactions.
The prevalence of CP in the general population is 3–5% and varies between individual climate zones [1]. The disease begins predominantly in adolescence or young adulthood and is more common in women than in men. There is a tendency towards familial aggregation of the disease.
There are primary and secondary SR. Primary, or idiopathic, SR is characterized by spasm of the digital arteries and thermoregulatory vessels of the skin when exposed to cold, without any signs of vascular damage. In secondary SR, a combination of Raynaud's syndrome with symptoms of other diseases is observed.
The hands are most often affected by SR. The main clinical sign of SR is a consistent change in color of the skin of the fingers in the cold. At the beginning of an attack of vasospasm, a pale coloration of the skin usually appears, after which within a few minutes the skin acquires a bluish-purple tint. Vasospasm usually lasts 15–20 minutes and ends with a rapid restoration of blood flow, as evidenced by the intense pink color of the skin (reactive hyperemia).
In some patients, attacks of vasospasm are accompanied by a feeling of freezing of the hands, numbness and tingling in the fingers, which disappear after blood flow is restored. In the phase of reactive hyperemia, patients may feel pain in the fingers.
In the early stages of the disease, changes in skin color may be observed on the distal phalanx of one or more fingers. In the future, the affected area covers all the fingers and possibly the feet, while the thumbs usually remain intact. Vessels of the skin of the face and other areas may also be subject to vasospasm. In these cases, characteristic changes in the color of the tip of the nose, lips and ears, as well as the skin over the knee joints can be observed. In some patients, the vessels of the tongue are also involved in the process, which manifests itself as dysarthria during an attack of vasospasm. During episodes of vasospasm, a marbling pattern may appear on the upper and lower extremities, a symptom called livedo reticularis. The frequency and duration of episodes of vasospasm can vary both in different patients and in the same patients at different times of the year (more intense in winter than in summer).
A three-phase change in skin color (whitening–blue–redness) is not detected in all cases; Some patients experience biphasic or single-phase color changes. Depending on the number of phases of skin color change, reliable and probable SR are distinguished.
- Reliable SR - repeated episodes of biphasic changes in skin color in the cold.
- Probable SR is a single-phase change in skin color accompanied by numbness or paresthesia when exposed to cold.
- There is no SR - there are no changes in skin color under the influence of cold.
In more than 80% of patients, primary SR is detected. To verify primary SR, diagnostic criteria proposed by EV Allen and GE Brown in 1932 and modified in recent years are used. These criteria, developed taking into account clinical and some laboratory parameters, as well as the results of capillaroscopy of the nail bed, include [2]:
- symmetry of episodes of vasospasm;
- absence of peripheral vascular diseases;
- absence of gangrene, digital scars or tissue damage;
- normal nail bed capillaries;
- absence of ANF and normal ESR.
The average age of development of CP is 14 years; only in 27% of patients the disease debuts at the age of over 40 years [3]. In primary SR, the symptoms of the disease are usually moderate, and only 12% of patients experience intense episodes of vasospasm [4]. In approximately 1/4 of patients, SR is detected among first-degree relatives [5].
However, with a large number of conditions and diseases associated with SR, it is considered secondary (table).
Secondary SR is most often associated with systemic scleroderma, systemic lupus erythematosus, other connective tissue diseases, hematological disorders and certain medications. Long-term observation of patients who had been given a preliminary diagnosis of primary SR revealed that 13% of them at a certain stage of the disease developed signs of systemic connective tissue disease (most often systemic scleroderma) [6].
Despite the identity of the clinical manifestations of primary and secondary SR, there are some differences in individual signs between these two conditions. The following signs indicate the likelihood of a secondary nature of SR:
- late age of onset;
- male gender;
- painful episodes of vasospasm with signs of tissue ischemia (ulceration);
- asymmetric nature of attacks;
- presence of signs of another disease;
- laboratory signs of autoimmune or vascular diseases;
- identification of ANF;
- reduction and dilatation of capillaries during capillaroscopy of the nail bed;
- widespread nature of SR, covering areas proximal to the fingers and toes.
Secondary SR usually develops over the age of 30 years and is characterized by more pronounced and painful episodes of vasospasm and structural changes in the capillaries [7]. ANF has a relatively low prognostic value for connective tissue diseases (30%), while the detection of specific autoantibodies significantly increases the likelihood of a secondary nature of SR [6, 8, 9]. Approximately 15–20% of patients with SR, who have specific autoantibodies and/or capillaroscopic changes, but no symptoms of connective tissue diseases, subsequently (usually within two years) develop one or another connective tissue disease [10, 11].
In all patients with newly diagnosed SR, it is necessary to conduct special studies for the purpose of differential diagnosis of the primary and secondary nature of the pathology.
First of all, you should clarify:
- whether the patient has symptoms of connective tissue diseases with which SR is most often associated (arthritis, myalgia, fever, dry syndrome, skin rash, cardiopulmonary disorders);
- whether the patient is taking any medications at the time of the study, especially chemotherapy drugs;
- whether the patient is exposed to vibration or other mechanical influences that injure the hands;
- whether episodes of Raynaud's syndrome are associated with certain positional changes.
It must be taken into account that clinical signs of SR-associated disease may develop several months or years after the onset of SR. The most objective and specific instrumental method for the differential diagnosis of primary and associated with systemic connective tissue diseases (primarily systemic scleroderma) SR is capillaroscopy of the nail bed. Normally, the capillaroscopic picture is a regular row of capillaries evenly distributed along the edge of the nail bed and of the same size. In systemic scleroderma, with which SR is most often associated, changes in the number of capillaries (reduction) and their size (dilation) appear early and often precede the development of clinical signs of the disease.
Differential diagnosis of SR
Increased sensitivity to cold is characteristic of the population as a whole. Cold skin or undefined mottled skin on the fingers, hands, and extremities is considered a normal response to cold exposure. In patients with SR, in addition to increased sensitivity, under the influence of cold, pallor and cyanosis of the distal parts of the fingers are occasionally observed. CP should be distinguished from acrocyanosis, a condition characterized by prolonged cyanosis of the hands or feet, which is aggravated by cold.
Increased sensitivity to cold can cause carpal tunnel syndrome and other neuropathies. In the differential diagnosis, conditions such as cryoproteinemia, dysproteinemia, contact with polyvinyl chloride, the presence of a tumor or hypothyroidism should be taken into account. If signs of the disease appear asymmetrically, it is necessary to conduct studies to identify occlusive diseases of large vessels. Atherosclerosis is not accompanied by typical symmetrical signs of SR, but in some cases it manifests itself as intermittent claudication during exercise, asymmetric limb damage, isolated or persistent digital ischemia. Vasculitis, emboli, or other occlusive vascular lesions can lead to critical ischemia, but not to the development of typical SR. There is evidence that SR may be a clinical manifestation of generalized vasospastic diseases such as Prinzmetal angina and migraine [12].
Livedo reticularis is also observed in vasculitis, antiphospholipid syndrome and occlusive diseases of peripheral vessels, in which, unlike SR, this symptom is stable.
Patients with peripheral vascular diseases, accompanied by decreased blood flow and ischemia, often complain of freezing of the extremities, numbness and tingling. In SR, unlike peripheral vascular diseases, these symptoms are observed only during vasospasm and disappear completely after restoration of the original blood flow.
Treatment of SR
General recommendations for patients with primary and secondary SR:
- Avoid prolonged exposure to the cold, including in unheated and damp rooms;
- it is necessary to wear mittens instead of gloves, which are worse at preserving heat, a hat and warm underwear;
- you should stop smoking, drinking coffee and caffeinated drinks;
- it is necessary to master techniques that can be used to reduce the duration of episodes of vasospasm (warming the hands in warm water or the axillary area, rapid circular movements of the hands, etc.).
Compliance with these recommendations is often sufficient for the treatment of patients with primary SR.
Digital arteries and thermoregulatory vessels of the skin are predominantly under sympathetic adrenergic control. Emotional stress can trigger digital vasospasm, and anxiety often exacerbates cold-induced Raynaud's attacks [13]. In such cases, it may be useful to prescribe sedatives. It is important to avoid the use of drugs that can cause vasoconstriction (sympathomimetics, clonidine, ergotamine, serotonin receptor agonists, etc.). Smoking can reduce digital blood flow, so patients with SR should give up this habit.
Drug treatment for SR
In cases of frequent and prolonged episodes of vasospasm in primary SR and in patients with secondary SR, drug therapy is necessary. To treat SR, drugs with a vasodilating effect or agents that affect the rheological properties of blood are used.
Calcium channel blockers
Calcium channel blockers have the greatest vasodilatory potential. The drugs of choice are dihydropyridine derivatives - nifedipine, amlodipine, isradipine and felodipine. Nifedipine, which has a short-term effect, in a single dose of 10–20 mg taken 3 times daily, significantly reduces the frequency and severity, and in some cases, the duration of episodes of vasospasm [15]. A single dose of 5–20 mg of nifedipine is quite effective in preventing cold-induced vasospasm when taken 15–20 minutes before exposure to cold. When nifedipine is prescribed, a significant increase in skin and muscle blood flow is observed [16]. Approximately 1/3 of patients while taking nifedipine develop side effects, the most common of which are arterial hypotension, headache, hyperemia, tachycardia, and swelling of the legs. Reducing side effects is possible by prescribing retard forms of nifedipine in a daily dose of 20–40 mg [17]. In patients with primary SR, compared to secondary, the therapeutic effect of the drug is usually more pronounced. With long-term use of nifedipine in large doses, paresthesia, muscle pain, as well as the development of tolerance and a decrease in the therapeutic effect of the drug are possible.
Along with nifedipine, other dihydropyridine derivatives are successfully used in the treatment of SR: amlodipine, isradipine and felodipine, which are long-acting drugs [18]. Amlodipine is prescribed once a day at a dose of 5 mg; if the effect is insufficient, the daily dose can be increased to 10 mg. The most common side effect of amlodipine is swelling of the ankles. Isradipine is prescribed at a dose of 2.5 mg 2 times a day. Side effects in the form of headaches and flushing are usually moderate in nature. Felodipine is used in a dose of 10 mg 1 time per day, mainly in the form of dosage forms that provide gradual release of the drug. Calcium channel blockers inhibit platelet activation, which also has a beneficial effect in SR [19].
If there are contraindications or intolerance to calcium channel blockers, vasodilators of other drug groups are used to treat SR.
The prescription of sympatholytic drugs is justified by the fact that adrenergic stimulation plays an important role in vasoconstriction. Prazosin significantly reduces the severity and frequency of vasospasm in patients with primary SR [20].
Prostaglandins have a complex physiological effect, in particular we are talking about vasodilation, antioxidant action, suppression of platelet aggregation, etc.
Alprostadil (vasaprostan), with daily intravenous infusions of 20–40 mcg of the drug in 200 ml of isotonic NaCl solution for 15–20 days, significantly reduces both the frequency and intensity of vasospasm in patients with primary and secondary SR [21].
Iloprost reduces the number of attacks per week and the intensity of vasospasm in patients with primary and secondary (associated with systemic scleroderma) SR by an average of 39 and 35%, respectively [22].
Pentoxifylline has antiaggregation and weak vasodilatory effects. Prescribed in combination with other vasodilators for a long time.
A number of vasodilators are used in the treatment of SR (transdermal nitroglycerin, hydralazine, papaverine, minoxidil), which can be effective in some patients. However, the frequent development of side effects (systemic hypotension, headache) limits the use of these drugs. The results of studies of the effectiveness of angiotensin-converting enzyme inhibitors in patients with SR are very contradictory; at present, drugs of this group are not widely used in clinical practice.
Xanthinol nicotinate is prescribed in tablets of 150 mg 3 times a day. The duration of administration, taking into account tolerability and contraindications to its use (as with other nicotinic acid preparations), is determined individually and is determined by the effectiveness and tolerability of the drug.
Drug therapy for SR has some limitations, including insufficient response, the development of tolerance with long-term use, and the development of a number of side effects, many of which lead to discontinuation of a particular drug. If conservative therapy is ineffective in reducing the manifestations of SR, surgical treatment is possible - local digital sympathectomy. However, the duration and expected severity of the therapeutic effect of sympathectomy have not yet been clarified, and therefore it is difficult to predict them. The expected effectiveness of sympathectomy can be assessed in the preoperative period using pharmacological sympathectomy.
In most cases, SR is a disease characterized by a favorable prognosis and a stable course. At the onset of the disease, especially in the presence of secondary risk factors for SR, all patients with SR are subject to medical examination and medical examination once a year. Patients should be warned about the need for an additional visit to the doctor if new symptoms appear that indicate the possible development of diseases with which SR is most often associated, primarily systemic connective tissue diseases.
For questions regarding literature, please contact the editor.
R. T. Alekperov, Doctor of Medical Sciences Institute of Rheumatology RAMS, Moscow
Symptoms of Raynaud's disease
Symptoms of the disease can begin quite suddenly, for example, after doing laundry or washing dishes in cold water, walking in the cold, sometimes after exposure to stress. Most often, 2-5 fingers and toes are affected, in more rare cases - other protruding parts of the body: ears, nose, chin and even tongue.
The attack is manifested by a sharp pallor of the fingers, they become white and very cold, then the skin color acquires a bluish tint, and after the end of the attack, the fingers become purple-bluish and painfully hot and swollen.
Over time, attacks become more frequent, can occur for no reason, and their duration increases to 2 hours.
Due to poor nutrition of the skin, the pads of the fingertips become flattened, the skin becomes dry, begins to peel, and hard-to-heal ulcers may appear around the nails. In severe cases, tissue necrosis can also begin - dry gangrene.
Examination of capillaries (capillaroscopy) in patients suffering from Raynaud's syndrome often does not reveal significant changes.
Raynaud's syndrome symptoms
What are the symptoms of Raynaud's syndrome , symptoms of Raynaud's disease , Raynaud's disease? With primary Raynaud's syndrome, a symmetrical lesion is noted, attacks are very frequent, and no background pathology is detected.
With secondary Raynaud's syndrome, a symmetrical or asymmetrical lesion is noted, only 1–2 fingers may be involved, trophic disorders are detected (onychopathy, ulcerations on the fingertips, gangrene, self-amputation of the fingers).
Diagnosis of Raynaud's syndrome
Since Raynaud's syndrome often occurs against the background of rheumatic and autoimmune diseases, laboratory research methods aimed at identifying them become important. The following types of tests are taken (for more details, see rheumatological examination):
- general blood test (increased ESR, decreased hemoglobin, leukopenia and thrombocytopenia are important);
- biochemical blood test (with Raynaud's syndrome, significant changes, as a rule, are not detected);
- coagulogram;
- general urine analysis;
- immunological blood tests (level of immunoglobulins, rheumatoid factor, cryoglobulins, various autoantibodies, for example, antinuclear antibodies, antibodies to DNA).
1 Treatment of Raynaud's disease
2 Reflexology (acupuncture)
3 Treatment of Raynaud's disease
Diagnostics
When the first signs appear that may indicate the development of Raynaud's syndrome, you should contact a vascular surgeon or rheumatologist. After collecting anamnesis, the specialist will prescribe the necessary examinations.
Since pathology is often a sign of various diseases, it is necessary to undergo diagnostics in order to identify them. For this purpose, laboratory tests are carried out. First of all, the indicators of a general blood test are important for determining the cause of the pathology. In particular, an increased ESR value, a downward deviation of the hemoglobin level from the norm, leukopenia and thrombocytopenia are important.
Also be sure to:
- Biochemical blood test, but in its indicators, as a rule, no significant changes are detected.
- Immunological blood tests, which help determine the level of immunoglobulins, various autoantibodies, etc.
- Coagulogram showing the level of blood clotting.
- General urine analysis.
Treatment of Raynaud's disease
Modern medical capabilities make it possible, if not to cure completely, then to significantly reduce the severity of the symptoms of Raynaud's disease. They use medication, physiotherapy, reflexology (acupuncture). Treatment of diseases that lead to the development of symptoms of Raynaud's syndrome is important.
Measures to prevent exacerbation of Raynaud's disease:
- to give up smoking;
- prevention of hypothermia (try not to overcool your hands, feet and face, dress according to the weather, make sure your shoes are dry, wear mittens in winter, etc.);
- adherence to sleep and rest patterns.
Highly qualified rheumatologists at MedicCity will help you cope with the manifestations of various rheumatological diseases. Our clinic diagnoses and treats rheumatoid arthritis, ankylosing spondylitis, reactive arthritis, gout, osteoarthrosis, osteoporosis, Sjogren's disease, systemic lupus erythematosus, systemic vasculitis, dermatomyositis, systemic scleroderma, rheumatism, etc. The most modern treatment methods are used. Trust the professionals!
Treatment of Raynaud's disease in Saratov, treatment of Raynaud's disease in Russia
Sarklinik provides comprehensive conservative treatment of Raynaud's disease in Russia on an outpatient basis. Treatment of Raynaud's disease in Saratov includes a variety of reflexology techniques.
Complex differentiated treatment of patients with Raynaud's disease in Russia at Sarklinik with the widespread use of new reflexology techniques allows one to achieve satisfactory results even with a severe clinical picture of the disease.
Sign up for a consultation. There are contraindications. Specialist consultation is required.
Photo: Millymanz | Dreamstime.com\Dreamstock.ru. The people depicted in the photo are models, do not suffer from the diseases described and/or all similarities are excluded.
Related posts:
Somatoform dysfunction of the autonomic nervous system treatment in Saratov
Migraine, migraine treatment in Saratov, symptoms, how to treat migraine, headache
Raynaud's syndrome, Raynaud's disease, symptom, phenomenon, treatment in Saratov, how to treat the disease
Solarite, solar plexitis, treatment of solaritis in Saratov
Comments ()
Treatment
Modern therapy has a sufficient list of possibilities for curing Raynaud's syndrome. Since the disease affects the vascular system, the need to maintain it and restore full functioning comes to the fore.
For this purpose, drug treatment methods are used:
- vasodilator drugs,
- medications that improve the chemical structure of the blood,
- calcium entry blockers.
The specialist prescribes the necessary medications depending on the situation. For an integrated approach, physiotherapy and dosed physical activity are also widely used.
Changes in the vascular network, although slowly, are treatable. However, one should not bring her condition to irreversible changes. Doctors recommend everyone to adhere to a reasonable lifestyle.
Raynaud's disease
Raynaud's disease - refers to vasospastic diseases, and is a special form of angiodystonia - angiotrophoneurosis with predominant damage to small terminal arteries and arterioles, characterized by paroxysmal local ischemia of the hands (usually fingers), sometimes feet, less often other parts of the body, leading in some cases to ischemic necrosis, formation of trophic ulcers, gangrene.
The disease is more common in young women and less common in men. The reasons are still not clear enough. The second and fourth fingers of the hands and feet are predominantly affected, in rare cases - other parts of the body that are exposed to cooling (nose, ears, chin).
The prognosis significantly depends on the timeliness of contacting a vascular surgeon, initiation of treatment and secondary prevention!
Complaints from patients with Raynaud's disease
Complaints depend on the stage of the disease. In the 1st stage, patients complain of burning, pain and paleness of the fingers, which usually occur during cooling and stress; in stage 2, complaints of blue fingers; in the 3rd stage for the appearance of blisters with bloody contents and trophic ulcers.
Diagnosis of Raynaud's disease
Diagnosis is made during an objective examination by a vascular surgeon, and is easily established by visible changes in skin color in areas of ischemia, a decrease in their temperature, and in severe cases, by characteristic secondary changes in the tissues of the fingers (ulcers and deformation of nails). Sometimes cold tests are performed, as well as ultrasonic scanning (USD) - examination (for thrombosis of the arteries of the forearm and shoulder), thermography, plethysmography and capillaroscopy.
Treatment of Raynaud's disease
Treatment is almost always conservative, less often surgical. Conservative methods include the use of vasodilator drugs. Drug therapy for Raynaud's disease continues throughout the patient's life, according to the scheme, and it should be taken into account that correctly selected therapy completely reduces the risk of complications. Surgical treatment includes sympathectomy or ganglionectomy.
Errors
Errors: Raynaud's disease is often confused with obliterating endarteritis, circulatory disorders in the limb (caused by compression of the subclavian artery) and other vasospastic pathologies.
Raynaud's disease is believed to be based on a genetic predisposition.
Risk factors provoke the onset of the disease: frequent and prolonged episodes of hypothermia of the hands, chronic trauma to the fingers, endocrine disorders (thyroid gland, gonads), as well as stress.
Stages of the progressive process
During the progressive process, there are 3 stages:
Stage I, angiospastic - characterized by short-term (several minutes) attacks of ischemia, usually occurring when cooling the hands (washing with cold water, rinsing clothes). The fingers become cold, alabaster-white (“dead finger”). Warming your hands helps, even if the attack was not provoked by cold, but by excitement, smoking or another factor. During the period of extinction of attacks, symptoms completely disappear (Fig. 1)
Stage II, angioparalytic, is characterized by an increase in the duration of attacks for more than an hour, their frequency and the development of cyanosis in the interictal period with the possible appearance of slight tissue swelling (Fig. 2).
Stage III, trophoparalytic, is characterized by pronounced changes in the tissues of the distal parts of the fingers, and then more widespread. Blisters with hemorrhagic contents form, necrotic changes and superficial trophic ulcers appear with dystrophic changes in the nails, and in severe cases, osteolysis with deformation of the affected phalanges of the fingers.
Treatment of Raynaud's syndrome
Effective treatment for Raynaud's disease must be comprehensive. First of all, it is necessary to eliminate the factors that provoke attacks.
The treatment program for the disease includes medication and physical therapy. In some cases, surgical treatment methods are indicated.
Drug therapy consists of:
- painkillers;
- vasodilators;
- anti-inflammatory drugs;
- antibacterial drugs;
- vitamin complexes.
Physiotherapeutic procedures for the treatment of Raynaud's disease include ultraviolet irradiation, galvanic baths, electrophoresis, etc.
Causes of Raynaud's disease
It is believed that the cause of excessively pronounced vasospasm in response to provoking stimuli is a defect in the central and local mechanisms of regulation of vascular tone. Among these factors, vascular endothelial, intravascular and neurovegetative disorders are important. In secondary SR, structural changes in blood vessels are also a significant factor.
Factors that provoke vasospastic reactions are low ambient temperature and/or emotional stress.
Symptoms
Raynaud's syndrome is accompanied by a sequential change in the color of the fingers (pale-blue-red), coldness, numbness, a feeling of pins and needles and sometimes pain in the hands. In addition to the extremities, similar manifestations can be observed in the area of the tip of the nose, chin, earlobes and tongue. The duration of the attack is usually 15-20 minutes.
Raynaud's syndrome is more common in women, with the first attack usually occurring before the age of 30. The syndrome is divided into primary - Raynaud's disease - and secondary, developing on the basis of concomitant diseases.