Brain tissue is represented by a wide range of formations. In terms of its structure, it is perhaps the most complex part of the human body, which determines the wide nature of the activity of the central nervous system. When assessing the structure, several areas of the central nervous system can be identified in this localization.
At the base of the cerebral structures is the so-called brain stem. It provides a group of vital functions: from breathing and cardiac activity to thermoregulation. Any damage or malfunction results in severe disability or death.
The pons is a component of the brainstem located between the midbrain and medulla oblongata, which ensures normal conduction of nerve impulses and makes it possible to perform a number of voluntary actions.
Responsible for some functions of higher activity. Its damage, for example, due to injury or stroke, leads to critical disruptions in the functioning of the entire body.
Diagnosis of lesions of this anatomical structure presents certain difficulties due to the deep and “inconvenient” localization. The only reliable method of examination is MRI or, less commonly, computed tomography.
Structure
The pons is located at the level of the brain stem and two main areas are conventionally distinguished in its anatomy.
- Top part. It consists of gray matter and includes several pairs of cranial nerves (from the 5th to the 8th). This is the actual functional structure.
- The lower or base - ensures the conduction of signals, acts as a transport route for natural impulses.
At the level of the upper part of the bridge there is a reticular formation. It is represented by a large accumulation of fibers that allow the entire central nervous system to function in a harmonious manner.
At the base there is a dense layer of thick conductive strands. They are three legs on each side, connected to the cerebellum and enable the extrapyramidal system to work.
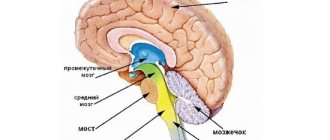
Below the pons is the medulla oblongata, in the upper part is the middle brain.
There are some differences in the structure of this education in children and adults. When evaluated in patients under 8 years of age, a complete absence of the myelin sheath is found, which is considered normal.
The development of this part of the brain is observed in early adolescence. The anatomy of the bridge is complex, which is explained by the need to carry out a number of actions on the part of the central nervous system.
Treatment
Constant monitoring of cyst size is necessary. If the patient has no complaints and no symptoms accompanying the anomaly, the therapy is focused on the cause that provoked the formation of the formation.
Fairy tale therapy is important
Medications used:
- Drugs to normalize blood circulation;
- Medicines against adhesions;
- Immunomodulatory agents;
- Antioxidants;
- Nootropics.
Constant monitoring of the patient's condition involves regular blood clotting and cholesterol tests, and monitoring blood pressure levels.
Surgery methods
When growth of the formation is observed, surgical intervention is prescribed:
- The endoscopic method is the least invasive, but can only be used for a certain location of the cyst.
- Trepanation is a very complicated operation, but it allows you to remove formations of any location and any size. Accompanied by a high risk of injury to brain tissue.
- During bypass surgery, a puncture is made and a tube is inserted to prevent the accumulation of cerebrospinal fluid. The method is accompanied by the risk of infection.
What functions does the bridge perform?
The pons is responsible for several important forms of activity.
Among them:
- Reflexive automatic and voluntary movements of the eyes and eardrum in response to loud sounds, as well as tissues of the oral cavity (palate). Any violation ends in problems.
- The ability for purposeful motor activity. Since the pons in the brain ensures the functioning of the cerebellum, any damage causes problems with the ability to control the body.
- Perception of vestibular stimuli. In this case, we are talking about the ability to perceive one’s body as a whole, its orientation and location in space, to respond to any changes in environmental conditions, and also to dampen unnecessary movements (for example, during sudden braking in public transport, stumbling, etc.). When affected, there is a lack of coordination. Ability to navigate in space.
- Providing olfactory function. The bridge has this ability partially. Other subcortical clusters are also responsible for it.
- Normal innervation of the skin and mucous membranes of the face.
- The pons is involved in the formation of sleep. This is a complex and coordinated work of several cerebral formations at once. Any violations immediately lead to problems with night rest. The patient becomes lethargic, asthenic processes appear.
- The functions of the pons include the acts of chewing and swallowing. Vital for nutrition and breathing.
- In fact, the body’s ability to perform normal gas exchange depends on the functioning of this structure. In the absence of adequate conduction of impulses, problems begin, even lethal disorders.
Basic actions are performed by nervous tissues constantly. Even minor changes are noticeable immediately.
The pons is part of the brain stem, therefore deviations in its activity become an indirect cause of dysfunction of this entire formation.
Complications, including rapid and fatal ones, are likely. High-quality medical care is not always possible due to the complex localization of structures and complex structure.
Other GM departments and their functions
The structure of the human brain is divided into several sections.
The formation of brain activity occurs during intrauterine development thanks to the rhomboid, midbrain, and forebrain.
The parts of our brain are responsible for various tasks, characterized by the telencephalon and medulla oblongata, intermediate and middle brain, as well as the hindbrain, pons and cerebellum.
Their functions are shown in the table:
| Medulla | Another name for this zone is the bulbus, located in the back of the skull, between the cerebellar region, the pons and the dorsal segment. The bulbus is a continuation of the spinal cord. The white matter of the brain in this area is represented by neurons, and the gray matter by nuclei:
If the functioning of this department is disrupted, heart problems will arise and the transmission of impulses to the brain centers will be disrupted. |
| Diencephalon | This brain region “filters” the impulses of neurons. It will accept all incoming data and decide where and how it will go next. It consists of a lower zone and a posterior zone, consisting of the epithalamus and thalamus. This department is responsible for the functioning of the endocrine system. The hypothalamus is part of the inferior region. This dense neuronal bundle regulates body temperature and the cycle of wakefulness and sleep. It synthesizes hormonal compounds that “tell” a person when to drink or eat. This is the pleasure zone, responsible for interest in the opposite sex. The medullary zone is connected to the pituitary gland, which regulates all glands. Impulses come from the hypothalamic zone to the pituitary gland, and the order to synthesize or stop the release of hormones is “executed.” The thalamus processes impulses from receptors responsible for vision, taste, hearing, and tactile sensitivity. The signals are distributed to the corresponding brain areas. The epithalamus synthesizes the melatonin hormone, which is responsible for the cyclic processes of wakefulness, the emotional sphere, and puberty. |
| Midbrain | The brain section is small in size and consists of two halves: on the roof in the subcortex there are centers of hearing and vision, and conductive pathways are located on the legs. This brain segment includes substantia nigra with red nuclei. There is a temporoparietal node and nuclei of neurons that control the ocular myofibers and temporal zones, which process sound effects that are transformed into recognizable sounds. Reflex activity and reaction to the stimulus are controlled. This organ is responsible for spatial orientation. |
| Finite brain | This is the youngest part of the brain, the main part of the brain, responsible for higher nervous activity, and has numerous grooves with convolutions. The corpus callosum separates the right and left hemisphere zones. Each hemisphere is equipped with a nucleus, mantle, and olfactory brain. |
| Pons | This anatomical formation is part of the hindbrain, which contains the cerebellar region. The functions of the bridge are similar to its name; it consists of nerve fibers. Through it there are impulses passing from the body to the GM and vice versa. It makes up the brain stem, located between the midbrain and medulla oblongata. It contains the nuclei of nerves that control chewing, facial expressions, and some ocular myofibers. It receives signals from receptors responsible for the sensory organs, skin, and inner ear. Thanks to this department, a person feels taste, maintains balance, and hears sounds. |
| Cerebellum | Consists of 2 hemispheric areas and an unpaired formation connecting them. The cerebellar surface is covered by the cortex, which forms 2 nuclei in the thickness of the hemispheric zones. In the deep layers, the lobules consist of a white substance that connects the cerebellar segment with three pairs of legs with the spinal trunk and GM. Responsible for coordinating and regulating the movements of myofibers and muscle memory. Thanks to him, a person maintains a certain body position. |
The anatomical and physiological parameters of the GM have been studied by scientists for decades; they are different for each person, because there are not even two people who think the same way. Experts will eventually reveal these and other secrets of the brain.
Pathologies that impair the functions of the bridge and their symptoms
There is a group of diseases that are typically characterized by disruption of the normal functioning of the body as a result of the destruction of the tissues in question.
Among them:
Brissot-Sicard syndrome
Accompanied by a disorder of cranial nerve activity. It is determined by unilateral paresis or complete paralysis of half the body.
The ability to control the muscles of the facial area is also lost, and ptosis (drooping of the eyelid) with impaired visual function is possible.
This disorder occurs against the background of an infectious, autoimmune or tumor lesion. Less commonly, it results from cerebral ischemia. After a transient attack or a full-fledged stroke.
Bonnier syndrome
Characterized by damage to a group of cranial nerves. In this case, the auditory and vestibular nuclei ultimately suffer.
Symptoms are nonspecific. Problems arise with the perception of sound stimuli. Patients constantly experience dizziness, nausea, and weakness.
Insomnia is also part of the clinic. The patient becomes irritable, and emotional instability is noted. Up to sudden changes in phases, as, for example, with bipolar affective psychosis.
Grenet's syndrome
A typical feature of this pathological process is a violation of the sensitivity of facial muscles, which ultimately leads to problems with the manifestation of non-verbal signals and emotions.
There is partial paresis of the masticatory muscles on one side. On the other hand, controllability impairment is also present, but to a much lesser extent.
Ventral syndrome
An extremely difficult condition. It is characterized by at least loss of speech function. This is the easiest case.
The classic situation is determined by the complete loss of the ability to move. The man cannot move. Communication is possible only through the eyes.
This disorder persists for a long time. Quickly leads to stagnation and death of the patient. Restoration is not possible.
Raymond-Sestan syndrome
Characterized by a key manifestation of the oculomotor nerves. A person loses the ability to voluntarily focus his gaze and move it from one object to another.
Spontaneous relief of the condition and its subsequent return for unclear reasons is possible.
Hübler's syndrome
There are no specific manifestations of blood paralysis of facial muscles. The facial expression is characterized as a mask.
The patient is unable to adequately non-verbally express emotions and respond to surrounding stimuli.
Skin sensitivity also decreases, which is detected by the results of functional tests and physical examination.
Foville syndrome
There is paralysis of facial muscles and strabismus with visual impairment.
Gasperini disease
Combined pathological process. Characterized by mixed symptoms.
Diseases leading to the development of syndromes
The structure of the Varoliev bridge suggests many possible lesions and an equally large number of manifestations. However, there is a group of diseases that become the foundation for the above syndromes.
This may include:
- Stroke. Acute disruption of cerebral blood flow in one area or another with death of nerve tissue and loss of some functions of cerebral structures. If the brain stem itself suffers, in the most favorable case it will end in a violation of higher activity.
- Ischemic transient attacks. Incorrectly called microstrokes. The same thing is observed, but there is no significant tissue death.
- Atherosclerosis of cerebral vessels. Impaired arterial patency as a result of blockage of the arteries by cholesterol plaques or spontaneous narrowing due to, for example, long-term smoking, hypertension (increased pressure).
- Infectious processes. Especially those that affect cerebral tissue. Encephalitis, meningitis.
- Demyelination. Multiple sclerosis.
The Varoliev bridge is responsible for a lot of important functions and has a systematic structure. Treatment of pathological conditions when the activity of this structure is already impaired is an extremely complex and sometimes impossible process.
Therefore, it makes sense to have a preventive effect on all diseases that may become a source of problems in the future. This is an important preventative measure.
Tumors of the medulla oblongata and pons
Treatment of cancer >> Books on oncology >> N. A. Popov, “Intracranial tumors” Len. dept. Medgiz Publishing House, Leningrad, 1961 OCR Wincancer.Ru Given with some abbreviations
Tumors of the medulla oblongata and pons are less common than other tumors of the posterior cranial fossa. Although their topical diagnosis usually does not present serious difficulties, at the onset of the disease it is possible to confuse them with other types of pathological processes, since tumors of this localization are rarely accompanied by a significant increase in intracranial pressure, and sometimes occur without cerebral symptoms. This is partly explained by the fact that patients often die before the conditions for intracranial hypertension are created.
A characteristic feature of tumors of this localization is the slowly increasing development of nuclear palsies of the cranial nerves (one or the other depending on the level of damage to the trunk) - in combination with cross conduction symptoms (pyramidal hemisyndrome and sensitivity disorders), i.e. alternating paralysis.
In contrast to their typical expression in vascular stem processes, in tumors of this type, paralysis is not so clearly defined, being, moreover, only a passing stage in the progressive development of the process. Soon they move to the other side or from the very beginning, to one degree or another, capture both halves of the trunk, which is more typical of tumors of the medulla oblongata.
Then the process may begin with damage to the nuclei of the cranial nerves (if the tumor grows dorsally), which is later joined by conduction disorders, or begin with the latter (if the tumor develops ventrally) with subsequent involvement of the cranial nerves. As a rule, the process ends with damage to the entire diameter at the level of maximum tumor development.
When the tumor is localized in the pons, the main symptom is damage to the trigeminal nerve with possible crossed hemihypesthesis or (with a more caudal localization) alternating paralysis of the facial nerve. A very striking symptom may be a violation of vestibular function in the form of sharp systematized dizziness due to damage to the nucleus of the vestibular nerve, which may make one suspect a tumor of the fourth ventricle, especially if there is also irritation of the vomiting center.
In cases of tumor growth within the medulla oblongata, severe bulbar disorders develop. There are often cerebellar symptoms due to the involvement of the cerebellar peduncles in the pathological process. They can be one of the early and clear signs of the disease, which often gives rise to an erroneous diagnosis of a tumor of the cerebellum or cerebellopontine angle. Due to the gliomas that often develop here and are relatively fast-flowing, it is possible that the tumor process may initially be mixed with others, such as inflammatory diseases (encephalitis), vascular diseases, multiple sclerosis, etc.
The difficulty of early and rapid recognition of brain stem tumors, as mentioned above, depends largely on the absence of cerebral symptoms, which are less common here than in other localizations, or appear late. However, T. M. Strelinskaya observed congestive nipples in half of her cases. If we take into account that tumors rarely develop in the brain stem, then at first, naturally, we have to think first of all about other diseases of the nervous system.
The prognosis of brain stem tumors is unfavorable, since surgical treatment is impossible: only radiotherapy can delay the steadily and usually rapidly progressing process.
Patient M., 10 years old, was admitted to the hospital on 17/X 1955 with complaints of headaches, sometimes with vomiting, a feeling of numbness in the right half of the body, and an unsteady gait. The pain began more than a year ago, but only recently became particularly intense. About two weeks ago, the patient began to notice that when turning her head to the left, a feeling of dizziness arose.
Objectively: Forced position of the head with a tilt to the right and slightly forward. The patient can only lie on the right side, otherwise severe dizziness occurs. The fundus, visual acuity and visual field were unchanged. Rotatory large-amplitude nystagmus, intensifying when looking up. Hypoesthesia of the left half of the face and scalp, the corneal reflex on the left is absent. VIII pair: auditory function without changes; caloric test: pronounced labyrinthine nystagmus, but no reactive miss. During the pointing test, the right hand spontaneously swings outwards.
The tongue deviates slightly to the right. Tendon reflexes are increased, on the legs they predominate on the right. Abdominal - not called. Decreased muscle tone in the right leg. Right-sided hemihypesthesia of skin sensitivity, with the exception of the face; deep sensitivity without changes. Performs coordination tests with uncertainty, adiedochokinesis in the right hand. The gait is unsteady with a deviation predominantly to the right and back; cannot stand on his right leg.
Craniogram without changes. Cerebrospinal fluid: protein - 0.033%o, cytosis - 0, ROE - 48 mm per hour. Clinical diagnosis: Tumor of the fourth ventricle arising from the upper half of the bottom of the rhomboid fossa. The patient was transferred to a neurosurgical clinic. Operation 30/XI 1955: Cloudy arachnoid adhesions in the area of the cistern magna were excised. Examination of the fourth ventricle revealed a tumor of the brain stem protruding from the bottom of the rhomboid fossa. A large amount of cerebrospinal fluid was released. Three weeks after the operation, horizontal gaze paresis to the left, paresis of the left facial nerve, right-sided hemiparesis and hemihypesthesia appeared. General cerebral symptoms and forced head position disappeared. Subsequently, tetraparesis, dysphagia, and dysarthria developed. On March 13, 1956, the patient died.
Section: Tumor of the pons (which is sharply changed and increased in size), protruding deeply into the greatly dilated IV ventricle, filling it almost completely. Histologically - glioblastoma multiforme.
In this observation, the tumor of the pons was taken to be a primary neoplasm of the fourth ventricle, which gave rise to surgical intervention. The most striking and important symptom in this case was the forced position of the head - a symptom so characteristic of intraventricular localization. Although this symptom was associated with attacks of severe dizziness in certain positions of the head, its dependence on disturbances in the circulation of cerebrospinal fluid, which occurs with neoplasms of the fourth ventricle, could not be excluded.
In a certain contradiction with this was the absence of typical Bruns syndrome, as a result of acutely occurring occlusive hydrocephalus. However, with tumors of the ventricle, dizziness can be very pronounced and even dominate the picture of the disease, being a focal symptom from the bottom of the rhomboid fossa. Then the pathogenesis of the forced position of the head can be understood as a manifestation of tonic reflexes on the neck muscles in connection with irritation of the vestibular apparatus at the bottom of the IV ventricle, i.e., as a phenomenon of a purely reflex nature.
The dependence of this symptom on the participation of secondary vestibular formations is supported by spontaneous bulbar nystagmus and caloric test data: the presence of pronounced thermal nystagmus in the absence of reactive overshoot, which indicated a break in the vestibular pathways from the nucleus to the cerebellum. This fact makes it possible to understand the mechanisms of vestibular dizziness in tumors of the trunk and fourth ventricle and make them dependent on the disinhibition of the function of the vestibular nerve; the auditory function is completely preserved (1).
Severe headaches, vomiting, and cerebellar symptoms could also indicate a tumor of the fourth ventricle; The participation of the trigeminal nerve did not contradict this, which is possible with tumors arising from the lateral indentation of the ventricle (I. Ya. Razdolsky). However, there was cross hemihypesthesia of pain and thermal sensitivity - a symptom that began with a feeling of paresthesia (numbness) as one of the early signs of the disease. This anamnestic fact was not properly assessed, which became obvious retrospectively: neither sensory nor motor conduction disorders are characteristic of tumors of the fourth ventricle, although they cannot be excluded (G. Cushing, I. Ya. Razdolsky).
The latter often observed severe dizziness depending on the position of the head and body. He considers isolated dizziness, as a nesting symptom, to be especially characteristic of tumors arising from the upper half of the rhomboid fossa. The author points out the significant difficulty of differential diagnosis of intrapontine tumors and the indicated part of the brain ventricle. The absence of symptoms from cranial nerves and motor conduction disorders at the onset of the disease also inclined the diagnosis more likely in favor of the ventricle rather than the brainstem.
Thus, the observation shows that the differential diagnosis of tumors of the brain stem and the fourth ventricle is sometimes very difficult and that a lesion of the dorsal pons involving the vestibular nuclei and forced position of the head can simulate a primary tumor of the fourth ventricle.
Patient B., 15 years old, was admitted to the hospital on 2/IX 1954 with complaints of severe double vision and headache. She has been ill since July 1954, but strabismus and diplopia appeared on 26/V 1954.
Objectively: General physical underdevelopment. There was no menstruation. Paresis of the left abducens nerve, diplopia. The fundus is unchanged. Convulsive contractions of the diaphragm occur periodically, which leads to involuntary noisy exhalation. Slightly unsteady, cerebellar gait. There are no motor, sensory or coordination disorders observed.
Cerebrospinal fluid leaked out in frequent drops; protein - 0.39%o, cytosis - 2/3. For 3 1/2 weeks (symptoms are described in sequential order - ——————————— 1 According to G.S. Zimmerman, a forced position of the head, as a consequence of tonic labyrinthine reflexes, is observed with damage to the oral parts of the brain trunk. ——————————— ity of their development) there was some difficulty in speech, absence of the pharyngeal reflex, smoothness of the left nasolabial fold. The girl began to exhibit some psychotic symptoms (lack of criticism of her own condition, depression, etc.). Drooping of the right palatal arch, choking when eating. The gait became unsteady, dizziness, a sensation of noise and ringing were observed, strabismus and diplopia intensified, and horizontal spontaneous nystagmus. Corneal reflexes are reduced.
Peripheral paresis of the left facial nerve, paresis of the soft palate. Diffuse muscle hypotonia, tendon reflexes in the legs are animated, bilateral Babinski's sign. In the left hand there is uncertainty during the finger-nose test, instability with a tendency to fall to the left, and a cerebellar gait. Increased headaches. The patient's condition progressively worsened, drowsiness appeared, and psychotic disorders intensified; the voice became aphonic, and bulbar symptoms increased. The fundus remained normal. Mild right-sided hemiparesis appeared. Violation of coordination tests on both sides.
X-ray of the skull: digital impressions, flattening of the sella turcica. Clinical diagnosis: Brain stem tumor. Operation 10/XI: Trepanation of the posterior cranial fossa, revision of the bottom of the fourth ventricle - no tumor was found. The cerebellar tonsils are lowered and flattened. After separation of the arachnoid adhesions, cerebrospinal fluid appeared. After surgery and radiotherapy, her general condition improved. The patient was discharged on January 22, 1955, and 3 months later she was admitted again in serious condition with apartria, involuntary urination, but still without motor and sensory conduction disorders (there was only anisoreflexia of the limbs and bilateral Babinski's sign). The patient died on 29/IV from bulbar palsy.
Section: The pons is greatly enlarged in volume, the tumor infiltrates mainly the base of the bridge, mainly on the left side; hemorrhages into the tumor tissue. Histologically - astrocytoma.
In this case, the first and for a long time the only symptom of the disease was paresis of the left abducens nerve (diplopia, strabismus); headaches came later, as did breathing problems and an unsteady gait. The fundus was normal. All this made me think at first about brainstem encephalitis. However, subsequent involvement in the pathological process of the facial, auditory and vagus nerves gave reason to suspect the presence of a tumor of the pons, which was facilitated by the appearance of psychotic symptoms (euphoria, moria), then drowsiness, lethargy and others. These disorders, in the absence of signs of intracranial hypertension, should be explained by obvious neurodynamic disturbances of cortical activity due to the presence of a lesion in the brain stem.
In addition to paralysis of the abducens nerve, the vagus nerve was affected, while the facial and auditory nerves were slightly affected (with complete preservation of vestibular function); there were also mild cerebellar symptoms. However, the patient did not have conduction (motor or sensory) disorders, therefore, there were no alternating paralysis. The latter are considered characteristic of brain stem tumors, but, as observation shows, they may not appear even at the height of the development of the disease.
The absence of paralysis of the limbs for a long time cast doubt on the diagnosis of a tumor of the trunk, despite damage to the cranial nerves. This circumstance did not allow us to exclude the possibility of a tumor of the fourth ventricle, especially since the first symptom was paresis of the abducens nerve, which, together with the facial nerve, is most often affected by tumors of the fourth ventricle emanating from the upper half of the rhomboid fossa (I. Ya. Razdolsky). This is what made the decision to undergo revision of the fourth ventricle. The descent of the cerebellar tonsils into the foramen magnum was apparently the cause of the bulbar symptoms.
Noteworthy is urinary retention at the height of the disease, which was then replaced by incontinence, despite the absence of motor pyramidal disorders. We also observed a similar fact in the case of cysticercus of the pons, and L. Ya. Pines and L. O. Sklyarchik in the case of a tumor of the pons (taken for encephalitis).
When comparing the clinical and anatomical data, the discrepancy between the severity of damage to the bridge and the clinic is striking: the almost complete absence of paralysis, despite the tumor predominantly affecting the base of the bridge, while clinical symptoms were observed mainly from the tegmentum - the nuclei of the cranial nerves. This is explained, according to A. N. Ageeva and E. P. Semenova, by the relative preservation of cells and myelin fibers not only in astrocytomas, but also in polymorphic cell glioblastomas. T. M. Strelinskaya and especially L. M. Dukhovnikova emphasize the possibility of a compensatory function of the cortex. This circumstance also contributes to difficulties and errors in the diagnosis of stem tumors. A. N. Ageeva points out that most of the cases she studied anatomically were diagnosed erroneously as a tumor of the cerebellum (cerebellopontine angle); the same fact is noted by E. P. Semenova.
Patient L., 27 years old, was admitted to the clinic I7/XII 1949 with complaints of headaches, speech disorder, and unsteady gait. Ill since early September 1949; in November, paresthesia in the left hand and mild swallowing disorders began to appear periodically. On November 28, the patient stopped working.
Objectively: The fundus of the eye is unchanged. Horizontal nystagmus of the eyeballs. The right corneal reflex is reduced, mild hypoesthesia and a feeling of numbness in the right half of the face. Peripheral paresis of the right facial nerve. Mild dysarthria and dysphagia. Slight left-sided hemiparesis with hyperreflexia, Babinski's sign and foot clonus. Abdominal reflexes are not evoked. Feeling of numbness in the left hand and slight intention tremor. The gait is ataxic. Over the course of two months, the painful phenomena progressed steadily.
Nine days later, there was an absence of the right corneal reflex, weakness of the masticatory muscles, an increase in the masseter reflex, a decrease in taste on the right side of the tongue, an increase in dysphagia and dysarthria and left-sided paresis of the limbs; mild hemihypesthesia, disturbance of coordination tests on both sides, and spastic-atactic gait appeared.
Cerebrospinal fluid: protein - 0.33%o, cytosis - 1/3. 23/I visual acuity and fundus are normal. There is a loss of symmetrical areas in the upper halves of the visual field - partial horizontal hemianopsia, and a narrowing of the visual field to colors along all meridians in its lower halves. Left-sided hemiplegia and right-sided hemiparesis with severe ataxia of the limbs. Aphonia. From 13/II there is paresis of the abducens nerve on the right, limited movements of the lower jaw, atrophy of the masticatory muscles, paralysis of the right facial nerve, decreased hearing on the right, a sharp limitation of tongue movements, paresis of the soft cabbage, and a sharp impairment of swallowing. Anarthria, tetraplegia, hyperpathia of the left half of the body; retention of urine and stool. 20/II the patient died. Clinical diagnosis: Spongioblastoma multiforme of the pons. The anatomical diagnosis is the same.
Recognizing the nature of the tumor and its location did not present any particular difficulties in this case, but at the onset of the disease the presence of symptoms such as nystagmus, dysarthria, paresthesia in the face and hand, increased and uneven tendon and absence of abdominal reflexes, cerebellar symptoms could be indicated in 27 -year-old patient with multiple sclerosis. This was the initial diagnosis. However, headaches, a rapid increase in previous symptoms and the appearance of new symptoms soon gave reason to suspect a tumor of the pons, which was confirmed by the entire further course of the disease. The rapid development of the process made the malignant nature of the neoplasm obvious. The absence of congestive nipples and other signs of increased intracranial pressure confirms the generally accepted idea of the rarity or later appearance of hypertensive symptoms in tumors of the pons. However, according to some data (T. M. Strelinskaya, A. N. Ageeva), they are observed quite often.
Noteworthy are the peculiar changes in the visual field: loss of symmetrical areas in the upper halves of the visual field to white and almost complete horizontal hemianopia to red - an unusual symptom for this localization. It develops in the terminal period of the disease along with tumor growth and is obviously caused by the dislocation of stem formations in the direction of both visual tracts; their compression can explain this kind of change in the visual field, which is generally very rare. (1)
A. N. Ageeva established significant dislocation of the brain stem in many cases of tumors of the pons. —————————————— 1 In the optic cords, such a grouping of fibers is allowed in which the upper and lower sections of the optic tracts are connected, respectively, to the upper and lower halves of the retinas of both eyes. —————————————— Secondary changes in the cerebral appendage due to vascular compression have been described, which led to the appearance of pituitary symptoms (Time). A.D. Dinaburg and D.L. Voloshchenko discovered the mixing of brain formations in the direction of the chiasmatic cistern.
It should be noted that in this, as in many other cases, changes in the visual field appear more clearly when examined with the help of colored marks. In addition, for the red color there is a narrowing along all meridians and the lower halves of the visual field, which confirms the actual existence of these visual disorders. Obviously, the appearance of this symptom is possible only in later stages of the disease, but detection of visual field defects then becomes especially difficult due to the serious condition of the patient.
Patient M., 32 years old, was admitted to the clinic on December 7, 1945, with complaints of attacks of headaches, sometimes with vomiting and involuntary urination, and blurred vision. She has been ill since the summer of 1943, when the above symptoms and short-term loss of consciousness first appeared. Since then, the mentioned attacks have been repeated at intervals of up to six months. In the spring of 1945, a convulsive attack developed; tapeworms (tapeworm) were discovered. Since September, decreased vision has been noted; in October, pain in the right half of the face and a feeling of numbness in the left hand, double vision and staggering when walking. Sometimes during attacks I experienced a peculiar sensation: “some kind of hot stream will flow deep in the forehead and the urge to stool immediately arises.” In November, the patient's condition noticeably worsened, and night and morning headaches appeared.
Objectively: Sharply expressed congestive nipples. The pupils are unchanged. Atrophy of the masticatory muscle and absence of the mandibular reflex on the right. Hyperesthesia in the area of innervation of the first and second branches of the right trigeminal nerve. Forced position of the head: the patient throws it back, sometimes tilting it to the right and supporting it with her hands. Slight neck stiffness, mild Kernig's sign. Slight left-sided hemiparesis, worsening after hypertensive attacks. Sensitivity is not impaired. Craniogram without changes.
Convulsive attack I2/XII with loss of consciousness; the muscle tone of the left arm is sharply increased, it is bent at the elbow joint, the left leg is in a state of extension; pulse weak, rare; face pale. After the attack, ptosis of the right eyelid, nasal tone of speech, and paresthesia in the right half of the face were observed. Clinical diagnosis: Cysticercosis of the brain (region of the pons, cerebellum). The patient died on December 18, 1945.
Section: On the right in the area of the putamen, in the optic thalamus and in the cortex of the inferior parietal lobule there are separate bubbles of the cysticercus. In the pons, at the level of the root of the fifth pair on the right, there is a single bubble, the size of a small hazelnut (well encapsulated, with a fin inside), forming a protrusion into the cavity of the fourth ventricle.
In this observation, it should be noted the very rapid development of the disease with severe hypertensive crises, which led the patient to death 11 days after admission. The diagnosis of cysticercosis was not in doubt, as was the localization of the process in the pons. Attacks of pain and paresthesia in the face were sometimes accompanied by paroxysmal disorders of complex visceral functions - urination and defecation, which are usually not observed with damage to this level. This indicates the possibility of the development of seizures with dysfunction of the bladder and rectum when the pons is damaged, as the clinic shows, apparently through a reflex pathway from the trigeminal nerve nucleus. The above once again indicates a very close functional relationship between the animal and autonomic nervous systems.
Doubts could arise when explaining movement disorders, namely seizures of unilateral tonic convulsions. The position of the limbs of the Wernicke-Mann type, which characterizes these convulsions, and transient post-seizure stem symptoms (ptosis, paresthesia in the facial area, paresis of the soft palate) undoubtedly indicated their stem origin.
The forced position of the head with its deviation back, which is rarely observed in general, and the Bruns symptom complex (in the absence of cerebral hydrocele) are apparently explained by the protrusion of the cysticercus bubble from the substance of the brain into the cavity of the fourth ventricle, which disrupted the circulation of the cerebrospinal fluid and thereby contributed to the occurrence of hypertensive crises. In this case, the position of the cysticercus bubble, generally rarely observed in the pons, explains the periodic nature of the occlusion of the Sylvian aqueduct at the site of its entry into the IV ventricle and thereby the onset of severe hypertensive crises.
Here, the possibility of a once living cysticercus of the fourth ventricle, which only later turned out to be “immured” in its bottom, cannot be excluded, as sometimes occurs in connection with reactive inflammation of the ependyma in the circumference of the bladder.
See further: Multiple brain tumors >>