September 24, 2019
36369
0
4 out of 5
Stenosis or pathological narrowing of the spinal canal is a dangerous disease that often accompanies intervertebral hernias and other spinal pathologies. It provokes severe back pain, paresis and paralysis, and stenosis of the spinal canal at the lumbar level can cause disruption of the pelvic organs and be accompanied by involuntary defecation and urination.
The disease seriously reduces the quality of life and threatens the development of severe complications. In a short time it can lead to compression myelopathy and myeloradiculopathy. Therefore, if symptoms of stenosis occur, treatment should be started immediately.
Types of spinal canal stenosis
There are several classifications of the disease. The main one was a change in the sagittal size of the spinal canal. Highlight:
- Absolute stenosis of the spinal canal is diagnosed when it narrows to 10 mm and its area reaches 75 sq. mm. This is invariably accompanied by compression of the nerve roots of the cauda equina.
- Relative - the size of the spinal canal is at least 12 mm, area - up to 100 square meters. mm. Signs of relative spinal canal stenosis appear when another factor is added that causes compression of the nerve endings.
A combination of absolute and relative stenosis of the spinal canal of the lumbar and cervical region is possible. In such situations they speak of a mixed form of pathology.
Depending on the location of the narrowing site, lateral and central stenosis are distinguished. In the first case, there is a decrease in the root canals to 4 mm, while in the second, there is a reduction in the distance from the posterior surface of the vertebral body to the base of the spinous process located opposite it.
There are also congenital and acquired forms of the disease. The first occurs as a result of exposure to infectious and toxic factors during intrauterine development of the fetus at 3–6 weeks. In such situations, moderately severe central spinal stenosis is more often diagnosed.
Acquired or secondary occurs when:
- injuries;
- degenerative-dystrophic changes in intervertebral discs and facet joints;
- spondylolysis;
- compaction of the yellow ligaments;
- Bekhterev's disease;
- undergoing spinal surgery;
- tumor processes, etc.
Secondary degenerative spinal stenosis can be either absolute or relative. More often it forms in the lumbosacral spine at the L5–S1 level. Depending on the cause of its development and accompanying signs, discogenic, discarthrogenic, etc. are distinguished.
Accurate determination of the type of pathology using an MRI examination allows you to choose the best treatment option and surgical technique. To obtain a complete picture, patients are also prescribed radiography and CT.
Adults and children can undergo a full diagnosis of the disease using the latest generation equipment from the specialists at SL Clinic. The vertebrologist will explain the diagnostic results in detail and, if necessary, select the optimal treatment tactics for the detected disorders. Since our neurologists, traumatologists - orthopedists and neurosurgeons work in close cooperation, our patients are completely protected from diagnostic errors and, if indications for surgical treatment arise, they will be immediately consulted about the possible options, consequences and risks.
Make an appointment with doctors at the Central Clinical Hospital of the Russian Academy of Sciences
The best specialists of the department of vertebrology
They receive patients with spinal canal stenoses of varying degrees of severity and origin.
The patient is examined directly on site, and an individual treatment program is developed for him, including drug therapy and physical therapy. In difficult cases, when absolute stenosis is accurately diagnosed, surgeons at the Central Clinical Hospital in Moscow
perform spinal surgeries, returning patients to motor activity and life without pain.
make an appointment
with
a vertebrologist, rheumatologist
or other musculoskeletal specialist by phone or using the online form.
Treatment methods
Spinal stenosis can be treated conservatively or surgically. But inexorable medical statistics indicate that only 32–45% of patients experience positive dynamics due to the use of medications, physiotherapy and exercise therapy. But even in such situations, treatment of stenosis without surgery does not lead to recovery, but only contributes to a slight improvement in the condition, especially if stenosis of the left or right root canal L5-S1 or another segment is diagnosed.
Conservative therapy includes:
- taking individually selected drugs from the group of NSAIDs, muscle relaxants, vitamins, drugs to improve blood flow, chondroprotectors, etc.;
- blockades with anesthetics;
- corticosteroid injections;
- phonophoresis;
- magnetic therapy;
- SMT therapy;
- Exercise therapy.
Therefore, today the only way to avoid the development of complications and achieve complete elimination of unpleasant symptoms is surgical treatment. Stenosis surgery is designed primarily to eliminate those factors that led to compression of the spinal cord and its nerve roots. For this purpose, decompression operations are performed. During these procedures, the herniated disc or vertebral arch that causes canal stenosis is removed. If necessary, stabilization of the spine is performed in order to fix the vertebrae in the anatomically correct position and avoid their displacement in the future, i.e., to prevent relapse.
Decompression interventions
Initially, decompression interventions are used to eliminate the effect of compression of the spinal canal. Today, in the arsenal of spinal surgeons there are 3 types of techniques that are used for disc herniation with stenosis, including L5-S1:
- Classic discectomy is an operation that involves removing the entire intervertebral disc through an incision of up to 10 cm. It is indicated for anterior compression of the spinal cord by a herniated protrusion of the intervertebral disc, including if there are 2 hernias and stenosis. Although there are more gentle methods for removing pathological formations, open discectomy leaves no chance for their re-formation in the same area of the spine, which completely eliminates the risk of relapse of the disease. A titanium implant (cage) is installed in place of the removed disc, providing reliable support for the vertebrae.
- Microsurgical discectomy - surgical intervention has the same goals as open surgery, but is carried out with special instruments through a miniature incision, the length of which does not exceed 3 cm. Therefore, after it, patients recover easier and faster. But microsurgical discectomy does not allow fixation of the vertebrae with anterior stabilization systems, which is necessary when spinal stenosis and hernia are interrelated.
- Decompression laminectomy – This operation is used for posterior compression of the spinal cord. It consists of partial removal of the vertebral arches in the affected area, followed by stabilization of the spinal column with special structures.
All types of surgical interventions are performed in the medical field. Some of the best spinal surgeons in Moscow are capable of performing operations of any degree of complexity, and the availability of modern equipment makes it possible not only to accurately pre-assess all the risks and potential benefits of each procedure, but also to perform it with precise accuracy.
Stabilizing interventions
After compression of the spinal cord is removed, surgeons must fix the spine in a physiological position and create optimal conditions for proper load distribution during physical work. Depending on the location of the narrowing, the following can be used:
- Systems that stabilize the anterior support columns are cages with bone chips.
- Posterior stabilization systems – used for fixed connection of vertebral bodies, titanium structures for transpedicular fixation.
Both options for stabilizing systems are considered the optimal treatment option for the disease. Interbody cages allow you to reliably fasten the anterior column of the spinal column and prevent relapse of the disease, and transpedicular implants reliably stabilize the spine, preventing it from moving.
Special dynamic stabilization systems are also used. There are several types of such structures, each of which has its own strictly limited scope. This:
- Interspinous U-implants – systems of this kind are designed for dynamic fixation of the spinous processes of the lumbar spine, including spinal canal stenosis at the level of L3–L4, L4–L5, which may be an indication for their installation. The U-system allows you to slightly reduce the load on the posterior support columns and increase the area of the spinal canal, thereby relieving pain caused by spondylous joints of the vertebra.
- A transpedicular fixation system with nontinol rods is also indicated for installation in the lumbar spine for reliable connection of adjacent vertebral bodies. This system makes it possible to maintain a large range of movements, due to which motor abilities are practically not limited.
- Dynamic interbody implant – designed for installation in place of a removed disc when spinal canal stenosis of the cervical or lumbar spine is diagnosed. Its design features allow you to maintain a fairly good range of motion.
Their disadvantage can be considered the impossibility of use in cases of spinal instability, since they do not provide a pronounced therapeutic effect and are unable to hold the vertebrae in the desired position. Also, over time, their mobility is lost.
Treatment
Conservative treatment of absolute stenosis is not used. It is ineffective due to the rapidly deteriorating condition of the patient. Self-administration of painkillers and ointments by patients is contraindicated, as this further aggravates the situation. The person does not feel pain, but pathological processes continue to progress .
Surgical treatment of the disease involves the use of the following types of operations:
- Decompressive laminectomy.
- Installation of vertebral stabilization systems.
- Application of interspinous fixation.
Decompression laminectomy
This method has been used since the days of Henk Wibster. It consists of removing those structures that cause compression . That is, resection of the spinous processes, vertebral arches, and affected joints is performed.
Laminectomy is used if severe compression of the spinal cord occurs
However, this type of intervention has a number of significant disadvantages. Namely, the removed structures constitute the third supporting column of the spine, and their resection leads to the development of instability. According to statistics, instability occurs in 45% of those operated on. In addition, the operation is performed using a posterior approach, in which the complication rate reaches 12.
If the cause of the stenosis is a hernia, then it is possible to perform a disectomy , that is, complete removal of the disc followed by its replacement with an implant.
Installation of stabilizing systems
Stabilizing operations are used as independent treatment or as a complement to laminectomy .
Recently, minimally invasive operations with access through small incisions have been used. Spinal stabilization as a method has a number of advantages, but is not without its disadvantages. When installing mechanisms, neighboring vertebrae are damaged, as a result, their mobility increases and related pathologies develop: spondylolisthesis, scoliosis.
Interspinous fixation
With stenosis, the load is redistributed from the anterior spinal support to the posterior one. Installation of clamps reduces the load on the posterior support and expands the lumen of the spinal canal .
The operation is performed through small incisions under microscope control. First, posterior decompression is performed, then an implant is inserted into the interspinous space. This preserves the possibility of flexion and extension of the spine.
Interspinous fixation allows you to distribute the load on the vertebrae
A positive outcome of the operation can be achieved in 85% of cases. At the same time, related diseases do not develop. The load on the joints is also reduced, the spine relaxes, and pain disappears.
Such operations are contraindicated in cases of vertebral instability , since the effect of the intervention is insufficient. In this case, it is advisable to use stabilizing operations. If stenosis has developed as a result of a vertebral hernia, then the optimal therapy is microdisectomy, which involves resection of the bone structure that caused the narrowing of the canal.
Rehabilitation
The most important stage of treatment is postoperative rehabilitation. Be sure to wear a support corset . Physiotherapy procedures are also required: ultrasound, electrical stimulation.
At the late rehabilitation stage, physical therapy and massage are included. Patients who have undergone surgery are recommended to undergo annual spa treatment. These activities are aimed at strengthening muscles, normalizing metabolism and preventing relapse.
Cervical decompression surgery
With cervical spinal stenosis, there are practically no symptoms. They begin to appear in advanced stages of the disease in the form of:
- severe pain in the neck on one or both sides, radiating to the shoulders, shoulder blades, arms and back of the head;
- painful spasms throughout the body;
- the appearance of numbness and weakness in the arms when moving the neck;
- the presence of a sensation of “goosebumps” on the skin of the upper extremities;
- breathing disorders when the pathology is localized at the C3–C4 level.
Surgical treatment of cervical spinal canal stenosis is performed through an anterior or posterior approach. The choice depends on the nature of the current situation and the presence of concomitant neck pathologies.
The operation to eliminate stenosis of the cervical spinal canal using an anterior approach involves making an incision on the frontal surface of the neck. It is performed from a microsurgical approach and is not traumatic; it requires a high level of skill from a vertebrologist. Usually the surgeon tries to make it in a natural fold of skin so that over time the postoperative scar becomes invisible.
Indications for this type of intervention are:
- kyphosis;
- anterior compression accurately determined on MRI;
- severe spinal instability;
- degenerative cervical spinal canal stenosis, involving more than 2 vertebrae.
The essence of treatment for neck stenosis is discectomy and spinal fusion. After removal of the intervertebral disc, an interbody implant is installed in its place, which securely holds the vertebrae.
Operations with a posterior approach are also less traumatic and therefore safe in experienced hands. Laminectomy or laminoplasty is expected; if indicated, spinal fusion can also be performed, and spinal stability is ensured by installing suitable structures.
Indications for performing surgery using a posterior approach are:
- confirmation by MRI results of posterior compression;
- congenital stenosis;
- cervical kyphosis;
- detection of ostification of the posterior or anterior longitudinal ligament.
Traditionally, all manipulations are performed through a posterior approach when osteoporosis, ligamentous insufficiency, or the risk of developing pseudarthrosis are diagnosed.
About the disease
Picture of the course of the disease
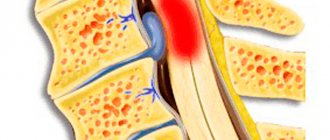
Absolute spinal canal stenosis is a narrowing of the canal lumen to several millimeters (less than 10). The narrowing occurs due to the pressure of the following elements: cartilage, bone processes, soft tissues. They invade the bone marrow space, causing compression and poor circulation. At the same time, the pressure of the vertebral hernia on the nerve endings is not stenosis.
Stenosis is characterized by narrowing of the spinal canal
Degrees and classification
From the point of view of origin, the disease can be congenital, acquired and mixed (a complex of congenital and acquired factors).
Several pathological factors are involved in the development of absolute stenosis : inflammation, ischemia and increased epidural pressure. Compression causes uneven blood flow and deterioration of oxygen supply to nerve endings. All this leads to the appearance of characteristic symptoms: pain, numbness, muscle weakness.
According to localization, three types are distinguished : stenosis of the cervical canal (c5-c6), thoracic and lumbar (I4-I5, I5-s1). Most often, pathology is detected in the lumbar region.
ICD code
According to ICD 10, the disease has code M48.
Prevalence
The disease occurs at any age, but people over 60 years of age are more likely to suffer. In them, the incidence of pathology reaches 35%, however, a quarter of patients do not feel any characteristic symptoms.
Decompression surgery for lumbar stenosis
Signs of lumbar spinal stenosis include gradually increasing pain in the back and legs. Initially, they appear during walking or physical work, but subsequently they can persist at rest. The discomfort does not have a clear localization, so patients often describe it as an unpleasant sensation in the legs. My legs ache especially at night. A symptom of restless legs appears.
Symptoms of lumbar spinal stenosis may also appear:
- increasing weakness in the legs when walking;
- lameness forcing the patient to stop and sit down;
- the onset of relief after bending the legs at the knees and hip joints, bending forward;
- numbness, the appearance of “pins and needles” in the legs;
- dysfunction of the pelvic organs, which is manifested by a sudden urge to urinate or defecate, decreased potency in men.
Before the development and introduction of spinal stabilization systems into spinal practice, treatment of lumbar spinal canal stenosis was carried out by decompressive laminectomy without fixation. Today, decompressive surgery in combination with fixation of the vertebrae with posterior or anterior stabilization systems is the gold standard.
For lumbar spinal canal stenosis, surgery is most often performed using transpedicular systems. Thanks to their installation, it is possible to achieve high functionality of the operated area and significantly reduce the rehabilitation period.
Statistical data also supports such systems. According to them, central and lateral lumbar spinal stenosis can be treated with 90% efficiency by posterior decompression followed by stabilization.
Signs of the disease
Stenosis has several characteristic signs. First of all, the functions of the spine and its tissues are disrupted.
- Swelling occurs in the damaged area due to tissue dysfunction.
- Hypoxia is another manifestation. It occurs because the tissues are compressed and oxygen does not flow through the blood in the required volume.
- The volume of the channel depends on the position of the body.
If treatment does not occur, the manifestations may worsen, which leads not only to disability due to failure of the spine, but also to pathological changes in all organs and systems. In severe cases, stenosis results in death as organs cannot function normally.
Treatment of complicated stenosis
The most common comorbidity is spinal instability. In such situations, the use of only interspinous fixation systems or decompression interventions is impossible. This will lead to increased loosening of the vertebrae and worsen the patient's condition. In such situations, only front and rear stabilization systems can be used.
If a patient is diagnosed with a L5-S1 hernia and spinal canal stenosis or protrusion in another segment, the “gold standard” of treatment includes 2 stages:
- Performing microdiscectomy or open discectomy in combination with the installation of transpedicular implants.
- Spinal stabilization with a titanium cage.
With timely surgery, patients have a high chance of a full recovery and return to a full life.
Treatment of spinal stenosis
Many factors go into determining the optimal way to perform surgery. We are talking about the location of the pathologically narrowed area on the spine, the cause of root compression, concomitant diseases of the patient, etc. Most often the problem is solved by:
- Endoscopic surgery.
- One-stage or two-stage operation with thoractomy.
- Operations involving the installation of implants – metal or from a person’s own bone tissue.
Features of rehabilitation
Once surgery is completed, patients are allowed to get up on their feet the same day or the next morning. During the normal course of the recovery period, discharge from the hospital occurs after 3–4 days. Each patient receives detailed recommendations from the doctor, strict adherence to which is the key to obtaining the most pronounced effect from the operations performed.
All patients are recommended:
- during the entire rehabilitation period, do not lift anything heavier than 3 kg;
- it is important to avoid vibration, shock, sudden movements, turns, and monotonous movements;
- Serious physical activity is unacceptable;
- Light household work is allowed, but if you experience pain, weakness or other symptoms, you should consult your doctor;
- on the recommendation of a doctor, it is necessary to begin performing special exercises and then regularly engage in exercise therapy under the guidance of a rehabilitation specialist;
- 4 weeks after surgery you should start swimming.
On average, the recovery period is 6–8 weeks. Accurate implementation of all medical recommendations allows you to reduce it and speed up the patient’s return to their usual lifestyle.
Children
Children, no less than adults, are susceptible to spinal diseases. In approximately 6% of cases of diagnosing stenosis, it is of a congenital nature. In other situations, narrowing of the spinal canal occurs due to degenerative changes and injuries. The peculiarities of the anatomy of a child’s body determine the possibility of developing pathology even as a result of falling from his own height onto his knees or somersaulting.
Therefore, often when examining previously absolutely healthy children who have recently complained of short-term weakness in the legs, spinal canal stenosis L4–S1 was discovered. The disease also often provokes scoliosis and spondylosis.
The main difficulty in treating children is early diagnosis of the disorder. Since they cannot always accurately describe what worries them, or do not attach due importance to alarming symptoms, parents may be unaware of the development of the disease for a long time. Patients are often referred for an MRI after undergoing a number of other studies carried out regarding emerging lameness or other manifestations of pathology.
Treatment of stenosis in children is carried out using conservative therapy. If it is ineffective or there is a risk of complications, the help of surgeons is required. In mild forms, non-surgical treatment often gives good results, but the presence of spinal column deformities almost always requires surgical interventions. They are aimed not only at eliminating stenosis, but also at eliminating the prerequisites for its development. Therefore, surgical treatment of spondylolisthesis and correction of scoliosis are often performed simultaneously or in several stages.
Causes of stenosis
A normal spinal canal provides sufficient space for the spinal cord and cauda equina. The narrowing of the canal that occurs with spinal stenosis can be congenital or acquired. Some people are born with a narrow spinal canal or have a curvature of the spine that puts pressure on the nerves, soft tissues, or ligaments. In the presence of a disease such as achondroplasia, improper formation of the bone tissue of the vertebrae occurs, thickening and shortening of the vertebral pedicles occurs, which leads to a narrowing of the spinal canal. Among the acquired reasons there are the following reasons.
Stenosis surgery
Our clinic performs a full range of surgical interventions indicated for stenosis, including the installation of transpedicular stabilization systems.
The cost of surgical treatment of stenosis starts from 450,000 rubles and depends on: - The implant manufacturer; — Clinic (where the operation will be performed) and the class of the ward. The price includes: — Stay at the clinic before and after surgery; — Implants. — Operation; - Anesthesia; — Postoperative observation. — Observation and consultation during the rehabilitation period. All clinic services and costs are shown in the price list