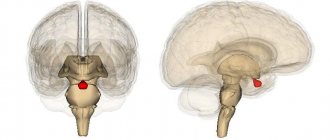
Craniopharyngioma is a rare type of brain tumor. It is localized in the pituitary gland. It is mainly first diagnosed in children aged 5-14 years or in adults over 40. The survival rate for craniopharyngioma for 10 years is about 90%. For a long time, the neoplasm does not manifest itself with any symptoms, but over time, multiple abnormalities develop: endocrinological, visual, hormonal.
Reasons for development
Craniopharyngioma develops due to excessive proliferation of epithelial cells in Rathke's pouch. It is formed in the fetus in the first trimester of pregnancy and is the basis for the future pituitary gland. If development occurs normally, then after the formation of the pituitary gland, Rathke cells are no longer produced. Craniopharyngioma appears only if this tissue continues to divide.
Typically, pituitary craniopharyngioma occurs due to a hereditary predisposition. A mutation of chromosomes occurs, which leads to the formation of a tumor. It can also occur due to intrauterine development disorders in the first trimester of pregnancy - this is when all the fetal organs are formed. This can be affected by taking medications, exposure to radiation, poisons and toxins.
Intrauterine infection and early severe toxicosis significantly increases the likelihood of craniopharyngioma. Chronic diseases of the mother, such as kidney pathologies, diabetes mellitus or tuberculosis, can contribute to the development of a tumor in a child.
Craniopharyngioma in children
Craniopharyngioma is uncommon in children. It is diagnosed in only 4% of all brain tumors. Typically, the first signs of the disease are diagnosed at the age of 5-14 years; craniopharyngioma occurs equally often in boys and girls. Initially, the pathology does not manifest itself with any obvious signs. Over time, the patient begins to complain of the following symptoms:
- Frequent headaches, worse in the morning;
- Nausea and vomiting;
- Delayed sexual and physical development;
- Violation of hormonal and endocrine functions;
- Change in behavior;
- Confusion;
- Visual impairment;
- Decreased appetite, increased thirst;
- Impaired motor functions;
- Increasing epilepsy;
- Swelling of the fundus;
- Altered psychopathological state.
Depending on the location of the tumor and its size, the manifestations of the disease may vary. It is important for parents to monitor the condition of their child, because timely diagnosed craniopharyngioma responds well to treatment.
Craniopharyngioma in adults
Craniopharyngioma is a benign tumor in the brain. Usually it begins during embryonic development and is localized in the hypothalamic-pituitary region. Due to the growth of the tumor, numerous cysts often form, inside which fluid from proteins and cholesterol accumulates. In this case, the papillary form of craniopharyngioma is mainly diagnosed in adults.
Suprasellar and intrasuprasellar craniopharyngioma
The initial classification of craniopharyngiomas was developed by V. Grekhov at the Institute of Neurosurgery named after. Burdenko. In the future, it was repeatedly detailed and changed. Today it is customary to distinguish the following topographic variants of craniopharyngiomas:
- Suprasellar
. Such tumors grow within the sella turcica, displacing the diaphragm. They can spread supra- and parasellar. The neoplasm develops from the remnants of the epithelium, which is preserved at the level of the pituitary gland; - Stem
. They spread in the area of the pituitary gland stalk, gradually affecting the bottom of the 3rd ventricle. They are localized above the sella turcica, displacing its diaphragm down; - Intra-extraventicular
. They develop at the level of the pituitary infundibulum and spread into the cavity of the third ventricle. This type of craniopharyngioma is associated with the accumulation of embryonic epithelium in the infundibulum area.
Adamantimatous and papillary craniopharyngioma
Craniopharyngiomas vary in structure. They may contain cysts or consist of dense tissue. Cystic formations are characterized by slow growth, extremely rarely their diameter exceeds 5 centimeters. Typically, such tumors have up to 50 cysts, in rare cases their number reaches 200. The formation itself is dense, with a strong capsule, and quickly connects with brain tissue and blood vessels.
NB!
Under the influence of various factors, the tissue structure of craniopharyngioma can change.
If craniopharyngioma has been present in the body for a long time, there is a risk of necrosis. This contributes to the rapid formation of cysts. Inside they are filled with liquid with a high lipid content. Craniopharyngiomas can vary in cytological structure. The following types of such tumors are distinguished:
- Adamantine-like
. Occurs in most cases. Mostly diagnosed in children. A neoplasm of this type consists of remnants of embryonic tissue. They mainly consist of cysts. Adamantine-like craniopharyngiomas are characterized by polymorphism; - Papillary
. It is mainly diagnosed in people over 40 years of age, and practically never occurs in children. Such a tumor consists of metaplastic cells, with virtually no fossilization. Papillary craniopharyngiomas can consist not only of epithelial but also epidermal cells. In such tumors, degenerative processes occur and cysts and stroma develop.
Cytohistological features
Structurally, craniopharyngiomas are divided into tumors consisting of dense tissue and containing cysts. The latter can be from two to five centimeters in diameter, in rare cases larger cysts form. They are characterized by slow growth.
As a rule, areas of cystic craniopharyngioma of the brain contain up to 50 cysts, but sometimes their number can reach two hundred. In appearance, these formations are yellow or clay-colored, with a dense capsule, well associated with the brain tissue and its vessels (the tumor is supplied with blood from the cerebral vascular basin).
Note. Over time, the tissue structure and morphological features of craniopharyngioma may change.
As it develops or when the tumor has been present for a long time, necrosis may form, which leads to cyst-forming processes. Cysts are filled with fluid with a large amount of lipids (up to 100%), the exudate may also contain fatty acids and cholesterol crystals. Salt deposits often form on the outside of the capsules.
The cytological structure of craniopharyngioma is represented by epithelial tissue with cells of varying degrees of differentiation. Depending on the structure, there are two types:
- Adamantine-like craniopharyngioma of the brain is diagnosed most often (about 85% of all tumors in this group). The tumor is more typical for childhood. Its tissues consist of the remains of embryonic tissues. Neoplasms of this type are characterized by polymorphism. They are compact (10% of cases), cystic (25-32%) and mixed (up to 60% of cases).
- Papillary craniopharyngioma of the brain is more typical for adults (30-40 years old); it is extremely rarely diagnosed in children. They account for approximately 15%. Cytologically it is represented by metaplastic cells. As a rule, neoplasias are solid, petrification is insignificant or absent.
In addition to cells of epithelial origin, craniopharyngiomas can be represented by epidermal epithelium. In tumors of this type, various degenerative processes, cysts, or stromal ossifications form. The tumor capsule is formed by connective or hyal tissue. Different types of histological structures can be considered as phases of craniopharyngiomas.
Symptoms
Craniopharyngioma of the pituitary gland is characterized by the development of endocrine and metabolic disorders, and intracranial hypertension syndrome. Because of this tumor, the balance of many hormones in the body is disrupted: gonadotropin, LH, ACTH, STH. This leads to the development of hypothyroidism, hypogonadism, hypocortisolism, and diabetes insipidus. Over time, hypothalamic-pituitary disorders occur, such as:
- Constant feeling of thirst;
- Polyuria, enuresis;
- Developmental delays, decreased growth rates in children;
- Rapid increase in body weight;
- Increased fatigue, muscle weakness;
- Menstruation irregularities, decreased libido.
The severity of such deviations depends on the location of the craniopharyngioma, its size and the age of the patient. Early symptoms of a tumor also include visual disturbances: decreased visual acuity, development of blindness. If the tumor is located in the third ventricle and compresses its openings, intracranial pressure increases - the patient complains of a constant headache.
NB!
The intensity of manifestation of pituitary craniopharyngioma depends not only on the size and location of the tumor. If the tumor is large, but it does not compress neighboring areas, the symptoms of the pathology may be minor.
Main signs and symptoms
About 80% of children with pituitary craniopharyngioma or another type of tumor have slower growth and developmental delays. During adolescence, patients experience either late or too early puberty. Often the disease is accompanied by osteoporosis - the destruction of bone tissue with rather slow generation and strengthening.
There are also symptoms that are practically independent of the age and other characteristics of the patient:
- excess weight, which is observed in 20% of cases;
- headaches and high intracranial pressure;
- optic nerve atrophy, decreased quality of vision;
- mental disorders (typical for the older age group).
As soon as you feel at least one of the listed signs, be sure to contact a neurologist or other doctor for diagnostics: x-rays, magnetic resonance imaging, biopsy, hormone tests.
Diagnostics
To diagnose craniopharyngioma, several studies are performed at once. This helps determine the possible cause of the pathology, its exact location, and the degree of damage to surrounding tissues. Standard diagnosis of craniopharyngioma includes the following measures:
- Anamnesis collection, visual examination of the patient
. The doctor will learn about the symptoms that concern the person, clarify the general state of health, and the presence of risk factors; - Biochemical and general blood tests
. Determine the concentration of vital blood components; - General urine analysis
. Determines kidney function, rate of urine excretion; - Hormonal blood test
. Determines the content of biochemically active substances and identifies deviations from the norm. The test allows you to diagnose endocrine disorders; - Neurological examination
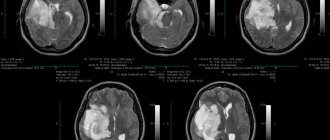
. The function of the brain, spinal cord, and nerve endings is assessed. The doctor needs to check the person’s muscle strength, memory, vision, hearing, reflexes, and coordination; - CT and MRI
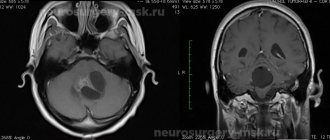
. Diagnostic imaging techniques that provide accurate images of the brain. This helps determine the size and location of the tumor and what tissues it has affected. MRI when determining pituitary craniopharyngioma gives a clearer picture; - Biopsy
. The most accurate examination method for craniopharyngioma. A portion of the tumor is removed using a needle for further histological examination. This determines the exact nature of the tissues.
NB!
When diagnosing pituitary craniopharyngioma, blood and urine tests are of high diagnostic value. Your doctor will need to check your electrolyte levels to help diagnose diabetes insipidus. It is also necessary to exclude germ cell tumors, for which the levels of alpha-fetoprotein (α-FP) and beta human chorionic gonadotropin (β-hCG) are determined.
Features of disease diagnosis
Diagnostic studies of cranipharyngioma, as in most cases of diagnosing intracranial neoplasms, are based on neurological studies performed by instrumental methods. In addition to instrumental research methods, in some cases hormonal studies are added to confirm doctors’ suspicions about the location of the tumor and its negative impact on the functionality of the pituitary gland and hypothalamus.
Cranipharyngioma
requires the following diagnostic methods, including basic neuroimaging techniques and additional tests. Visualization of the tumor is achieved using magnetic resonance imaging, which makes it possible to view the tumor from different sides and from different angles. MRI studies provide the opportunity to visually identify changes in the structure of areas of the brain that have been displaced as a result of the development of a neoplasm. In addition to MRI studies, computed tomography is also important. With the help of CT, it is possible to establish the process of calcification in the body of the tumor, which threatens to develop into a severe form of pathology.
After identifying the location of the tumor, the patient is prescribed a series of laboratory tests to determine the functional capacity of the pituitary gland and the level of hormones in the patient’s blood. In addition, during the diagnostic process, the patient undergoes an examination by an ophthalmologist, assessing the condition and quality of vision.
Treatment
The basic treatment for pituitary craniopharyngioma is chemotherapy. It is carried out both as the main part of therapy and as an auxiliary part during surgical excision of the tumor. The radioactive drug is injected intravenously or into the spinal canal (in the case of surgical removal of a tumor, in its bed). Craniopharyngiomas cysts are filled with interferon preparations: they have a cytotoxic effect. Due to this, the process of self-destruction of tumor cells is started.
Craniopharyngiomas are prone to recurrence. And even after surgical interventions, many patients may develop a new formation within the first year. Because of this, they always undergo postoperative radiation therapy, which reduces the risk of such a consequence by 2 times. Today, the following methods show the greatest effectiveness in the treatment of pituitary craniopharyngiomas:
- Proton therapy
. Heavily charged particles are used that release all the energy into the tumor. Due to such targeted irradiation, it is possible to stop the growth of the tumor and also destroy some of the cells. The advantage of this technique is its highly precise action: the surrounding brain tissue is not irradiated; - Intracavitary radiotherapy
. This is one of the methods of radiotherapy in which the radiation source is located directly in the tumor. This avoids damage to the cranial nerves, blood vessels, pituitary gland and hypothalamus.
Therapy for pituitary craniopharyngioma in children
If pituitary craniopharyngioma is detected in children under 3 years of age, and the tumor is accompanied by the spread of numerous cysts, then a catheter is implanted in the pituitary gland area. Drainage of the cyst is organized, due to which its size is reduced. Nearby tissues and blood vessels are no longer compressed, and the symptoms of the pathology disappear.
Cyst catheterization is a minimally invasive method for treating pituitary craniopharyngioma. To increase the accuracy of the intervention, stereotactic settings are used. To remove cysts, a sclerosing agent may be injected into them. The walls of the tumor stick together, the tumor stops accumulating fluid. This technique is used exclusively in young children; in the future, more radical intervention is necessary: radiation therapy or surgical excision.
In older children, craniopharyngiomas are removed with a gamma knife. This is one of the methods of stereotactic radiosurgery, characterized by extreme targeting accuracy. High-dose radiation therapy is performed to remove the tumor. In this case, the surrounding tissues are not affected.
Types of operations to remove craniopharyngioma
Surgical treatment is the most effective method of treating cerebral craniopharyngioma
. The operation is quite complex: it has technical difficulties due to limited accessibility to the tumor. There is also a risk of damage to the pituitary gland, optic nerves, carotid arteries, and the floor of the third ventricle - all of these tissues are located in close proximity. The surgeon needs to remove all tumor tissue and not affect healthy cavities.
Radical tumor removal reduces the risk of relapse by up to 20%. In the future, postoperative radiation therapy can minimize the likelihood of future tumors. Currently, the following surgical techniques are used for pituitary craniopharyngioma:
- Surgery with craniotomy access with traditional opening of the cranial bones
. All manipulations are determined in advance using computer planning. This allows the operation to be performed as carefully as possible, preserving all surrounding tissues and formations; - Operation with transsphenoidal approach
. This is an endoscopic type of intervention. Small incisions are made under the nose and sinuses of the sphenoid bones, through which a neuroendoscope is inserted into the brain cavity. This minimally invasive intervention is easier for patients to tolerate and the rehabilitation period is shortened. But it must be taken into account that not all craniopharyngiomas are suitable for such an operation. Interventions with a transsphenoidal approach are performed only when the tumor is located suprasellar.
Craniopharyngiomas
Craniopharyngiomas (CP) account for 2.5-4% of all brain tumors; Moreover, about 50% of cases occur in childhood. Peak occurrence: age 5-10 years. They arise from the anterior superior edge of the pituitary gland; they are lined with stratified squamous epithelium. Some CFs may occur primarily in the third ventricle. Almost all CFs have dense and cystic components; The fluid in cysts varies, but usually contains cholesterol crystals. CFs are benign tumors and do not undergo malignant transformation. However, the difficulty in removing them makes their course prone to frequent relapses and the need for regular monitoring and repeated surgical and radiation interventions.
What clinical manifestations are characteristic of craniopharyngiomas?
Due to the involvement of the hypothalamic-pituitary system in the pathological process, patients develop a wide variety of disorders - diabetes insipidus, hypopituitarism with typical growth retardation (in children), visual impairment (due to a primary effect on the visual pathways and secondary to intracranial hypertension), hydrocephalus . Localization is a determining factor in the difficulty of radical tumor removal, the high frequency of relapses and the need for combined treatment (radiation therapy and radiosurgery), and hormone replacement therapy.
Are there any peculiarities in the diagnosis of craniopharyngeomas?
The method of choice in diagnosing CF is an endocrinological examination in combination with MRI of the brain without and with contrast enhancement. A frequent phenomenon on SCT of the brain without contrast and even on plain craniograms is the presence of calcifications in the chiasmatic-sellar region - in children in 85% of cases, in adults in 40%.
What treatment methods are used for craniopharyngiomas?
Surgical removal is the method of first choice in the treatment of newly diagnosed CF, because These tumors, as a rule, are diagnosed already in the presence of a detailed clinical picture against the background of a large tumor size. When removing giant craniopharyngiomas, mortality can reach 5-10%, mainly due to damage to the hypothalamic structures. Small craniopharyngiomas are amenable to surgical removal via a transnasal transsphenoidal approach using neuroendoscopic techniques. Most relapses occur within 1 year, with fewer occurring >3 years (very late relapses occur in cases where “total” excision was intended). With repeated operations, the number of complications and mortality are higher.
Stereotactic radiosurgery is the treatment of choice for the treatment of small recurrent craniopharyngiomas in both children and adults. CF tumors are quite radiosensitive and do not require high doses of radiation. In most cases, even close proximity of the visual pathways does not limit the possibility of effective treatment of the tumor.
Stereotactic radiotherapy is indicated for large CF recurrences (more than 3 cm), persistent recurrence after surgical treatment and/or impossibility of surgical removal. It is carried out in hypofractionation or standard fractionation modes.
Conducting conventional radiation therapy is considered unjustified due to the high risk of endocrine disorders, optic neuritis, and dementia.
In all cases of stereotactic irradiation, cystic craniopharyngiomas can significantly increase in size due to post-radiation changes (not to be confused with continued growth!), which, under conditions of functional saturation of this anatomical area, may require puncture or transnasal emptying of the tumor cyst. This effect is not typical for solid tumors.
Postoperative changes after removal of craniopharyngioma
Almost all patients with craniopharyngioma experience complications that impair quality of life. Such consequences can arise either due to the tumor itself or as a result of treatment. Patients often encounter the following problems:
- Loss of vision;
- The appearance of mood swings;
- Emotional disorders;
- Memory impairment;
- Endocrine dysfunction;
- Development of metabolic syndrome;
- Pathologies of blood vessels.
The pituitary gland is the main gland in the human body. It is she who is responsible for the production of basic hormones, and also controls the work of other organs and endocrine glands. If a person's pituitary gland function is impaired, multiple problems arise: obesity, decreased bone mineral density, deterioration of the lipid profile, decreased fertility. This often occurs even in those patients who adhere to hormone replacement therapy.
Due to damage to the hypothalamus, multiple hormonal changes also occur. And this affects the quality of life. The patient begins to complain of increased appetite, his body weight rapidly increases, his behavior changes, and his personality becomes emotional. Metabolic syndrome often develops - a group of disorders accompanied by obesity, elevated levels of triglycerides and cholesterol, and high blood pressure. Metabolic syndrome significantly increases the likelihood of strokes and heart attacks.
In most cases, treatment for pituitary craniopharyngioma requires surgery or radiation therapy. After such events, the likelihood of disorders of the blood vessels of the brain increases significantly. The risk of aneurysms and stroke increases, seizures and cognitive impairment often occur.
Due to the high risk of complications associated with pituitary craniopharyngioma, the patient must be under constant medical supervision. Only timely diagnosis will make it possible to identify the deviation at the initial stages and stop it. Social and psychological assistance will help improve the patient's condition. The specialist will tell the person how to competently cope with the experience, how to get rid of anxiety and minimize the risk of depression.
Prognosis and prevention
At the moment, doctors have not developed an unambiguous system for determining the stage of craniopharyngioma. The tumor can be newly diagnosed or recurrent. This is a benign neoplasm that is not prone to spreading to other parts of the brain. Despite this, they can cause numerous abnormalities in the body’s functioning: disruption of endocrine functions, damage to the optic nerve.
The 10-year survival rate for patients with pituitary craniopharyngioma is 90%. With adequate treatment, it is possible to preserve both the quality and life expectancy of the patient. If after radiation therapy the tumor continues to progress, they are completely removed.
It is impossible to completely protect yourself from pituitary craniopharyngioma. The disease has a hereditary predisposition. The only way to reduce the likelihood of developing pathology is to prevent the exacerbation of diseases in the mother during pregnancy, avoid self-medication with medications, and protect against the influence of toxins and poisons.
Treatment of craniopharyngioma
Craniopharyngioma belongs to a number of benign tumors, therefore it has several treatment options:
- Radiosurgery using cyberknife and gamma knife technology is used in clinics in Israel and Germany for complete tumor removal. Radiation therapy is used to prevent tumor progression. After radiation therapy, the patient should be monitored for about five years and undergo MRI and CT scans twice a year to monitor the tumor volume.
- The most traditional method of treating craniopharyngioma is surgery. Particularly relevant for large tumor volumes, when the use of radiosurgery is impossible. When treating craniopharyngioma, surgery gives the most encouraging prognosis.
- Very often it is impossible to completely remove the tumor due to the close location of the tumor body to the optic nerves and other vital structures. After surgery, the cyberknife technique is used or the remaining tumor is removed using radiation and hormonal therapy.
- Hormone therapy is used as a method of stabilizing the disruption of pituitary hormones.
conclusions
Craniopharyngioma is a benign neoplasm of the pituitary gland. Mostly occurs in children 5-14 years old. The disease develops due to disorders that occur in the fetus in the first trimester of pregnancy. In the initial stages, it is difficult to diagnose, because the pathology does not manifest itself with any symptoms for a long time. Treatment for pituitary craniopharyngioma is mainly surgical.
If you suspect pituitary craniopharyngioma in yourself or cannot recover from this disease, then feel free to contact the doctors of our medical center. They will conduct extensive diagnostics, develop an individual treatment regimen and monitor all stages of therapy.