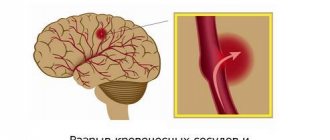
Symptoms of cerebral aneurysm
A small protrusion of blood vessels (less than 11-12 cm) has virtually no symptoms. The patient experiences discomfort only when the protrusion of the cerebral arteries has increased in size.
| Type of intervention | Price |
| Endovascular embolization of cerebral aneurysm | 450,000 - 600,000 rub. |
Medium (12-26 mm) and large (from 26 mm) aneurysms are characterized by a number of symptoms.
Among them:
- deterioration of hearing and vision,
- pupil dilation,
- partial numbness of the facial muscles.
Pronounced symptoms of brain damage appear when an aneurysm ruptures.
The patient experiences:
- nausea,
- acute pain in the temples, occipital and frontal parts of the head.
Often the patient cannot speak or swallow. When an aneurysm ruptures, the functioning of the vestibular apparatus is disrupted and vital functions of the body are lost. In addition, spasms and convulsions occur. The patient may fall into a coma. These symptoms are also associated with brain damage.
Important!
Treatment of an aneurysm through surgery should not be delayed. It should be understood that the pathology is very dangerous. The patient can die at any minute. It is extremely difficult to save him, especially if there is no way to quickly get medical help.
If you are diagnosed with a cerebral aneurysm, you should immediately contact a specialist for treatment.
Methods for removing a cerebral aneurysm
If you don't have symptoms and are at increased risk of rupture, you don't necessarily need therapy. In such cases, regular diagnosis of brain aneurysm is carried out: control CT or MRI studies are prescribed over time every 1-3 years. However, the decision for or against prophylactic shutdown of the aneurysm is, of course, made by you, based on the doctor’s recommendation. Therefore, when choosing a clinic or doctor, the latter’s specialization and experience play a decisive role.
If a cerebral aneurysm ruptures, surgery is inevitable. The tactics of surgical access are chosen by the neurosurgeon himself. Today there are two methods:
- clipping - open craniotomy operation;
- coiling - endovascular embolization.
Clipping of a vascular aneurysm of the brain
A traditional method in which a neurosurgeon makes a hole in the skull. Through this hole, he identifies the artery on which the aneurysm has formed and clamps the neck of the aneurysm with a special titanium clip. This allows you to turn off the aneurysm from the bloodstream and prevent its further growth or rupture.
Open surgery is now rarely resorted to and only in extreme cases (with rupture and heavy hemorrhage), since after clipping of a cerebral aneurysm there is an increased risk of disability.
Boiling
Unlike open surgery, the endovascular method is minimally invasive and involves shutting off the cerebral aneurysm from the inside using miniature platinum coils and without opening the skull. The patient is hospitalized (registered as a hospitalist) as a rule, the day before surgery. On this day, routine preoperative procedures are performed:
- ECG;
- blood pressure measurement;
- blood analysis;
- diagnostic angiography.
Within the framework of the latter, the exact location, volume and shape of the aneurysm is determined, and a 3D image of the vessels is formed. This allows the neurosurgeon to design the course of the planned operation. During the operation itself, the patient is under general anesthesia, access is carried out through puncture of the femoral artery with the introduction of a cannula approximately 2-4 mm thick (guidewire) through it.
Then a catheter is inserted through it, allowing the vessel to be monitored, thereby controlling the progress of surgical procedures. In addition to the guidewire, a minicatheter with a diameter of up to 0.5 mm is also inserted there. With the help of the latter, direct access to the aneurysm is provided and the coiling itself is installed, that is, a spiral is formed from platinum wire with a diameter of up to 0.25 mm.
For large aneurysms, there may be several coils. This allows you to fill the saccular space of the aneurysm from the inside, until it is completely excluded from the bloodstream. After surgery, without blood supply, the cerebral aneurysm ceases to be active , no longer poses a risk of rupture, gradually becomes overgrown with connective tissue, and decreases in size until it completely dries out. If the vessel lumen is wide, a stent is installed first, and then coil embolization. This allows you to strengthen the fragile vessel and protect it from possible perforation during the coiling process. Upon completion of the operation, all auxiliary instruments are removed and the inguinal artery is closed. The patient spends one night in the intensive care unit and, in the absence of complaints, is discharged a day later.
Risk group. Danger of aneurysm
An aneurysm is a disease of the arteries of the brain that is found in various people, regardless of age.
The risk group includes:
- smoking,
- alcohol abusers,
- patients with hypertension, hereditary vascular pathologies.
The insidiousness of an aneurysm is that in the early stages the symptoms of brain damage are almost invisible. It is not easy to notice them, especially for a constantly busy person. At the same time, a relatively small number of people undergo comprehensive examinations of the brain and blood vessels.
Many patients do not pay attention to headaches and nausea. Usually these conditions are associated with chronic fatigue and age.
Important! 25% of patients suffering from protrusion of the wall of a cerebral vessel die.
Request a call back Get a free consultation
Treatment of pathology
Emergency treatment for patients with a ruptured brain aneurysm includes restoring deteriorating breathing and reducing intracranial pressure.
There are 2 main treatment options.
They allow you to fasten the intracranial protrusion of cerebral vessels.
- Surgical clipping.
- Endovascular embolization.
If possible, treatment is given within the first 24 hours after bleeding to close the ruptured aneurysm and reduce the risk of recurrences that affect the blood vessels.
Let's consider the features of both methods.
Surgical clipping
The goal of the intervention is to apply a special clip to the neck of the aneurysm. This allows you to exclude it from the general bloodstream without blocking a normal vessel. If the aneurysm cannot be clipped, alternative techniques are used (wrapping, tripping, etc.).
Important! The operation to clip the cerebral vessels is performed with craniotomy. Microsurgical techniques are used to carry out the intervention. This allows you to free the aneurysm (its neck) from the feeding vessels. Complications after surgery arise from a previous rupture. Eliminating all its consequences is not so easy. When treating unruptured aneurysms, complications occur less frequently (in 4-10% of cases).
Request a call back Get a free consultation
Rupture of cerebral aneurysms, treatment
Modern methods of treating cerebral aneurysms are radically divided into two types of surgical interventions:
Operations involving opening the cranial cavity (craniotomy). Aneurysm clipping. Refers to extremely complex intracranial interventions. The purpose of the operation is to turn off the aneurysm from the bloodstream while maintaining the patency of the carrier and surrounding vessels, removing blood from the subarachnoid space of the brain. To minimize the consequences of the intervention, the optimal surgical approach is selected, microsurgical techniques and simultaneous clipping of the aneurysm neck are used. The operation is performed using an operating microscope and specially designed microsurgical instruments.
Endovascular interventions are operations without opening the cranial cavity, through a puncture of the femoral artery. The purpose of these interventions is to close the lumen of the vessel formed as a result of amyopathy and exclude it from the blood circulation. This is done with the help of microspirals, balloons and other agents that are delivered to the problem area and lead to thrombolization of the vessel. Since this method is minimally invasive and has fewer consequences, it is actively used in Germany, where in 90% of cases aneurysm is treated with these methods.
If the cause of a hemorrhagic stroke was a rupture of a cerebral aneurysm, and if this disease was diagnosed, then timely surgical treatment returns the person to normal life.
Embolization
This technique has become widespread in the last 15 years. It allows you to exclude the damaged vessel from the cerebral circulatory system without opening the skull. A special catheter is inserted through one of the veins or arteries. It moves through the circulatory system until it reaches the aneurysm. After this, using special instruments, the vessel is disconnected from blood circulation.
Embolization is the least traumatic way to eliminate aneurysms. That is why it has become widespread. Efficiency and advantages of treating cerebral aneurysm using modern endovascular techniques Embolization is a method that has proven to be highly effective.
That is why it is often used to disconnect a cerebral vessel from the circulatory system when:
- Inaccessibility of the aneurysm.
- Risk of serious complications with direct intervention.
- Carrying out operations on elderly people.
- Treatment of patients in serious condition.
Intervention is also prescribed when the aneurysm cannot be clipped.
Over the past few years, a large number of interventions have been performed. Moreover, surgery on cerebral vessels was prescribed even for gigantic aneurysms. The majority of patients did not require a long stay in the intensive care unit and were discharged from the clinic within 2-3 days.
There was no damage to any major healthy cerebral vessel. Thanks to this, patients were able to lead a normal life and did not experience any restrictions.
In some patients, the aneurysm was not completely excluded from the bloodstream during one intervention. In this case, another operation was performed. Repeated intervention on the cerebral vessels did not lead to a worsening of the patient's condition.
Main advantages of the method
- Low probability of need for repeated interventions. The operation is performed a second time in approximately 1 case out of 300.
- Possibilities for intervention to stop a cerebral vessel in patients who are contraindicated for extensive surgical clipping.
- Short duration of the procedure. Usually the operation takes no more than 2-3 hours.
- Opportunities for full recovery of health. An aneurysm will not bother you.
5. Immediate improvement. After intervention on a cerebral vessel, patients recover as quickly as possible. Moreover, embolization of cerebral vessels does not prevent them from leading a normal life.
Indications and timing of surgery for cerebral aneurysm
The indication for surgery for a cerebral aneurysm is the very presence of an aneurysm, even if it is small and asymptomatic. Patients with aneurysms literally live on a powder keg that can “explode” at any moment. Stress and constant worry from awareness of this risk can provoke pressure fluctuations and vasospasm, thereby bringing the moment of rupture closer, so if the operation is postponed, it will not be for a long time.
Only in rare cases can doctors adopt a wait-and-see approach: when the aneurysm is very small, located deep, and the operation can cause more harm, weeks after its presence, however, as practice shows, often the doctor’s indecisiveness and delay play a negative role - the pathology progresses and rupture follows.
Unruptured aneurysms require planned surgical treatment in neurosurgery or the vascular department, and it is important that it is performed by specialists with sufficient experience in such interventions, and that the clinic has minimal mortality and disability rates among patients.
Often patients who have been diagnosed with an aneurysm are themselves tormented by the question: to do or not to have surgery? Having heard and read a lot about the possible consequences of treatment, fearing neurological complications from the intervention, they seriously think about refusing it. In such cases, it is still worth thinking not so much about the risks of a planned operation, which can be minimally invasive and safe, but about the likelihood of hemorrhage with completely different negative statistics.
ruptured brain aneurysm
A ruptured aneurysm must be subject to surgical correction, but there are some differences in the timing of its completion, which are associated with the individual characteristics of the course of the pathology.
In the most acute and acute period of hemorrhage (the first two weeks from the moment of rupture), the following are considered indications for surgery:
- A rupture occurred with an uncomplicated course of the pathology;
- The patient's condition is stable;
- High risk of re-hemorrhage;
- The threat of severe vascular spasm and, as a consequence, cerebral ischemia.
During this period, patients in severe and critical condition undergo surgery only for life-saving reasons - compression of the brain, displacement of stem structures, acute hydrocephalus, massive foci of necrosis of brain tissue. In other cases, the operation is postponed until the condition has stabilized.
After the first 14 days from the moment of bleeding from the aneurysm, the operation is performed on patients:
- In serious condition due to a complicated course (severe vasospasm);
- With aneurysms that are difficult to access for removal.
Repeated hemorrhage is one of the most dangerous complications, which gives extremely high mortality rates, and therefore requires emergency surgical care. If the patient’s condition is so severe that the operation is extremely risky, then observation is carried out in the neuroreanimation unit, providing palliative care - drainage of the ventricles to reduce pressure in the skull.
The issue of surgical treatment of ruptured aneurysms with severe cerebral ischemia remains open and controversial; clear indications for surgery in such patients have not yet been precisely defined. Intervention and general anesthesia can aggravate damage to brain tissue, so surgery is performed immediately only in cases of compensated vasospasm; in other cases, wait-and-see tactics are used.