What it is?
Myelitis refers to all inflammatory processes of the spinal cord affecting the gray and white matter , or any spinal inflammation. They can be primary and secondary; the causes of primary processes, which are viral in nature, largely remain a mystery.
Myelitis is an inflammation of the inner and outer parts of the spinal cord
Secondary myelitis can manifest itself as complications of many diseases - measles, scarlet fever, typhoid fever, influenza, HIV infection, tuberculosis, syphilis and others.
The severity of the symptoms of the disease varies and depends on the form and its prevalence, but in any case it is severe, difficult to cure, and is fraught with serious complications. Sources of infection and the poisons (toxins) they release, entering the spinal cord through the lymphatic and circulatory system, lead to inflammatory and dystrophic abnormalities in it. Viral myelitis affects the spinal membranes, roots and nerve endings.
Picture of the course of the disease
Factors causing the disease lead to swelling of the spinal cord . Its beginning is considered to be the moment when the pathological process is launched, the next stage of which is the appearance of blood clots in the vessels due to circulatory disorders. And this leads to worsening swelling, i.e. the neurological process proceeds in an unbreakable circle.
Partial or (in some areas) even complete circulatory disorder provokes maceration (softening) and death (necrosis) of tissue . During the process of rehabilitation after an illness, areas of necrosis grow with connective tissue, i.e. transform into scars.
Scar tissue is unable to function, which causes pathological abnormalities (some or many) to become permanent. The spinal substance remains swollen, replete with infiltrates and hemorrhages, loses elasticity, and the “butterfly” retains its vague outline.
Classification
In most cases, the exact cause of myelitis is not known, but the factors that provoke it have been identified.
Diseases are classified according to etiology or cause of occurrence into four types:
- Infectious . This is the most common form, because observed in almost half of patients. It is divided into primary, when the infection initially entered the spinal cord, and secondary. In this case, inflammation of the spinal cord is a complication of another disease. Infectious myelitis is most often of a viral nature, sometimes it is provoked by a meningococcal infection. Secondary infection is often observed with osteomyelitis of the spine or due to infection through the blood when the whole body is affected. In addition to general intoxication, in these cases symptoms of a specific viral or bacterial disease also appear. For example, with measles it is a cough and a characteristic rash.
- Intoxication myelitis in many cases is a consequence of acute or chronic poisoning (harmful production) with salts of heavy metals, solvents, and alcohols.
- Traumatic – due to spinal injury. This includes mechanical damage or compression of the spinal cord with disruption of its functions, and possible penetration of infection into the spinal canal through an open wound.
- Neuroallergic (autonomic) . It is caused by systemic diseases, for example, in multiple sclerosis, myelitis is one of the signs of the disease. It also manifests itself in the early stages of the appearance of cancerous tumors.
| Based on the location of the source of inflammation in a particular spinal region, myelitis is divided into: | By degree of distribution: |
|
|
Myelitis can be classified depending on which part of the brain is inflamed
Prevalence
This disease, fortunately, is not considered common, because... occurs in 5 people out of a million .
The disease may be preceded by a short-term prodrome with general malaise, weakness, and muscle-joint pain. Usually, before damage to the spinal cord, there is a rise in body temperature, the appearance of radiculoneuritic pain syndrome, and short-term difficulty urinating. Paresthesia in the extremities is also quite typical. Spinal lesion syndrome can occur acutely, stroke-like, or increase gradually over 1 to 3 days. Acute transverse lesion of the spinal cord is accompanied by the development of spinal shock (diaschisis) with inhibition of reflex activity below the lesion. In this regard, for several days and sometimes weeks, muscle hypotonia, tendon areflexia, and the absence of pathological reflexes and spinal automatisms are observed. Only later does true spasticity appear in the paralyzed limbs. With a higher localization of the focus, the signs of spinal shock are more clearly expressed and are observed for a longer time.
The clinical picture of myelitis depends on the severity of the development of the process, as well as on the localization of the lesion and the extent of the lesion both across the diameter and along the length of the spinal cord. Moreover, in the first 2-3 weeks of the disease, with swelling and compression of the spinal cord, a picture of a complete transverse lesion appears, and only later the true extent of the process is revealed. The most common myelitis is localized in the thoracic segments of the spinal cord.
Symptoms of myelitis consist of segmental and conduction disorders. Paresis and paralysis can be of peripheral or central origin (with spastic type muscle hypertension, high tendon reflexes, expansion of reflexogenic zones, foot clonus). Pathological extensor reflexes on the legs (Babinsky, Oppenheim, Schaeffer, etc. reflexes) appear in the first days of the disease, and flexion reflexes (Rossolimo reflex) - after 10-14 days. Usually, especially with lesions located in the cervical and thoracic segments of the spinal cord, protective reflexes are clearly expressed, on the basis of which contractures are subsequently formed. Sensitivity disorders in transverse myelitis are conductive in nature, and all types of sensitivity are lost. The upper limit of sensitivity disorders is located 1-2 segments below the upper limit of the spinal lesion. In the area of sensitivity disturbances, skin reflexes disappear. In the first days of the disease, there is usually a delay in urination and defecation. Only with the lumbosacral localization of the myelitic focus does peripheral paresis of the sphincters occur with true urinary and fecal incontinence. In cases where the elasticity of the bladder neck is preserved, paradoxical urination occurs. In the future, with central disorders, urination and defecation are carried out automatically. The accumulation of residual urine in the bladder creates a constant threat of uroseptic complications. With transverse myelitis, trophic disorders in the form of bedsores are more or less pronounced, which can become secondarily infected and cause the development of sepsis and intoxication.
If the inflammatory focus does not cover the entire diameter of the spinal cord, then the spinal symptoms are much less pronounced. When half of the spinal cord is affected, Brown-Séquard syndrome develops with paresis and impairment of deep and partially tactile sensitivity on the side of the lesion and loss of pain and temperature sensitivity on the opposite side. In the presence of several foci, disseminated myelitis is diagnosed, when spinal pathology is combined with cerebral pathology - encephalomyelitis, with simultaneous damage to the spinal cord and spinal roots and nerves - myelopolyradiculoneuritis. In the latter case, symptoms of spinal damage are revealed only as the polyradiculoneuritis component decreases.
During myelitis, several periods are distinguished. The acute period of myelitis is characterized by an increase in symptoms and lasts from several days to 2-3 weeks. The early recovery period begins when symptoms stabilize. Its duration is usually 5-6 months. At this time, there is a regression of neurological pathology, sometimes quite intense. Favorable prognostic signs in this period are the closure of bedsores and restoration of the functions of the pelvic organs. This is followed by a late recovery period and a period of residual effects.
Infectious myelitis should be distinguished from recurrent encephalomyelitis and multiple sclerosis. The latter are characterized not only by symptoms of spinal damage, but also by symptoms of damage to the brain, and often to the optic nerves, rapid recovery and a relapsing course.
Differential diagnosis of myelitis and a spinal tumor is based on the slow increase in symptoms of tumors, the sequence of appearance of syndromes, the presence of pain and complete or partial block of the spinal subarachnoid space, detected during CSF tests.
Pathoanatomical picture of myelitis: the affected areas of the spinal cord are macroscopically flabby and have a grayish color; the characteristic transverse pattern of the spinal cord is blurred; the inflammatory focus can occupy its entire diameter; multiple lesions located at different levels are usually small in size. Microscopically, vascular disorders, inflammatory infiltration, degenerative changes in neurons, fragmented disintegration of nerve fibers and their sheaths below the lesion, which can spread to several segments, are noted. Subsequently, cysts and scars form in place of the dead nervous tissue.
Risk factors, causes
In addition to the etiology of the disease already listed, there is also a risk of damage to the spinal cord for the following reasons:
- allergy to the vaccine during vaccination;
- as a consequence of treatment of a malignant tumor with radiation.
- A disruption of the immune system, when the tissues of the spinal cord are not perceived as “our own”, and protection against them is activated with the production of antibodies.
There are no patterns in the risk of getting it based on gender and age. But some sources believe that teenagers 10-20 years old and older people are more often susceptible to myelitis.
Consequences
Did you know that...
Next fact
If the course of the disease is unfavorable, the following complications of the disease are possible::
- Bedsores - due to deterioration of skin nutrition in long-term bedridden patients.
- Contractures are a disorder of joint mobility in paralyzed limbs.
- Inability to restore the functions of organs and systems due to scar changes in the spinal canal: paralysis, incontinence.
The consequences of the disease depend on the severity of its course, the localization of foci and the degree of their spread . So, if after 3 months there is no improvement, then the patient faces disability or even death. The most dangerous for the patient’s life is the localization of inflammation in the cervical spinal cord, and if other parts of it are affected, this can lead to paralysis of the limbs.
Video: “How the spinal cord works”
Myelitis after a new coronavirus infection
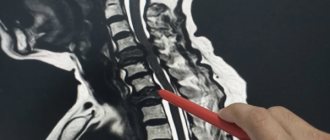
Myelitis (inflammation of the spinal cord) is a fairly rare neurological disease that can be caused by injury or infection. Most often, 1-2 segments of the spinal cord are involved in the process. I would like to share a clinical observation of a patient with myelitis that developed after suffering a new coronavirus infection. The peculiarity of this clinical case is the widespread level of spinal cord damage and the complete lack of response to therapy.
Patient L., 58 years old, suffered a new coronavirus infection from April 9 to April 20, 2020, the smear on April 20 was negative. Afterwards, he began to notice numbness in his legs, cold feet, and then a gradual increase in weakness in the lower extremities. On June 30, due to severe weakness in the legs, he called a doctor. The symptoms were regarded as manifestations of dorsopathy, the prescribed treatment (muscle relaxants, NSAIDs) was without effect. 07/04/20 to 07/03/20 was hospitalized in the neurointensive care unit of a city hospital, then transferred to the neurological department. A lumbar puncture was performed, and a CT scan of the brain was performed without pathology. The condition is regarded as chronic inflammatory demyelinating polyradiculoneuropathy. On July 13, 2020, for further examination and treatment, he was transferred to the neurological department of Clinical Hospital No. 1. During the initial examination, the neurological status noted lower flaccid paraparesis to plegia, decreased muscle tone in the lower extremities, and inconclusive sensory disturbances from the Th10-Th11 level according to the conduction type. The following examinations were carried out: ENMG - no evidence of damage to peripheral nerves was obtained, MRI of the thoracic spine: diffuse myelitis was detected, MRI of the lumbar spine: signs of myelitis. The patient was consulted by a neurosurgeon: diffuse myelitis, most likely of viral (coronavirus) etiology. Neurosurgical treatment is not indicated. Consulted with an infectious disease specialist: diffuse myelitis, most likely of viral (coronavirus) etiology. Pulse therapy with Solu Medrol 1000 mg No. 7, antibacterial therapy with Meronem, and complex vascular-metabolic therapy were carried out. Contrary to expectations, during the therapy, the patient’s condition and well-being showed no significant changes in the neurological status. The control MRI dated July 27, 2020 showed negative dynamics in the form of increased heterogeneity of the MR signal (increased volume of cloud-like areas of hyperintense MR signal on T2, STIR VI) from the spinal cord along its entire length. A course of plasmapheresis was started. Subsequently, the patient continued therapy in the neurology department with rehabilitation wards. An MRI of the brain, cervical spine, and thoracic spine was performed with contrast - there was no accumulation of contrast. On August 6, 2020, the patient was discharged with severe neurological deficit (lower paraplegia, pelvic disorders) with recommendations to continue supportive hormone therapy on an outpatient basis.
Symptoms and diagnostic methods
The symptoms of myelitis change at different stages of the disease. The primary manifestations of its infectious form are similar to other infectious diseases. This is a sharp increase in temperature to high numbers, chills, weakness.
Then they become more specific:
- Back pain , which is often not local in nature, but spreads to other parts of the body. This occurs due to the involvement of the spinal cord roots in the inflammatory process, as in radiculitis. This symptom quickly becomes acute.
Pay attention to the symptoms of myelitis. If the cervical part of the spinal cord is damaged, this is paresis (muscle weakening), and if the phrenic nerve is damaged, there is a risk of respiratory arrest. Inflammation of the upper part of the cervical spine is especially dangerous, threatening disorders of the medulla oblongata. And localization of the process in the lower part of the cervical region is dangerous due to persistent motor dysfunctions.- Damage to the thoracic part of the spinal cord, which is more common than other types, is characterized by spastic paralysis of the legs with muscle hypertonicity and cramps.
- Damage to the lumbosacral portion of the spinal cord is characterized by paresis in the legs and dysfunction of the pelvic muscles (incontinence). Muscles deprived of normal nutrition and regulation (due to nerve damage) gradually atrophy.
- Sensitivity disorders below the site of inflammation . This is a complete absence of pain, insensitivity to touch, cold, etc.
Diagnosis often relies on data from various spinal punctures (spinal fluid analysis). MRI of the spine and myelography are also used. These methods, together with symptoms and history, in most cases are sufficient to determine an accurate diagnosis.
Find out more about other spinal infections:
- To learn about spinal spondylodiscitis, follow this link
- Symptoms and treatment of spinal epidural abscess of the spine
- What is spinal discitis and what is the clinical picture of the disease, is described in the following article
- You can learn more about the diagnosis and treatment of Pott's disease on the page
- You can find out whether spinal tuberculosis is contagious or not here
Myelitis
DEFINITION, ETIOLOGY AND PATHOGENESIS
An inflammatory process involving the tissue of the spinal cord, caused by the presence of microorganisms in the nervous tissue of the spinal cord. The cause is most often a viral infection: enteroviruses (Coxsackie A and B, ECHO, polio, enteroviruses types 70 and 71), herpes viruses (HSV, VZV, CMV, EBV), HIV. May accompany neuroborreliosis, leptospirosis, syphilis and central nervous system tuberculosis. up
CLINICAL PICTURE AND NATURAL COURSE to top
May begin with severe back pain and/or pain in the lumbosacral region.
1. Inflammation of the anterior horns of the spinal cord: currently mainly caused by enteroviruses; sudden, progressive, asymmetrical flaccid paralysis, often of 4 limbs with muscle weakness, persists for several days, accompanied by fever and muscle pain; sensory disturbances do not occur. Changes in the medulla oblongata → dysphagia and respiratory failure.
2. Inflammation of the white matter, transverse myelitis: ascending flaccid paralysis, sensory disorders and sphincter functions.
3. Myelitis accompanying meningitis and/or encephalitis: a combination of symptoms characteristic of certain clinical syndromes and, in some patients, symptoms of a specific viral infection (however, their absence does not exclude the diagnosis).
Many patients are left with persistent neurological disorders: dysesthesia, paresis or paralysis of varying degrees and extent. Delaying treatment increases the risk of permanent damage.
DIAGNOSTICS up
In every patient with suspected myelitis, an MRI should be performed as early as possible (it also makes it possible to exclude non-inflammatory changes and compression of the spinal cord). Microbiological and serological studies, as in encephalitis → section. 18.6.2 and for meningitis →section. 18.6.1. In general analysis of the CSF there are inflammatory changes; with viral inflammation, the number of mononuclear cells is usually increased and the protein concentration is significantly increased (with poliomyelitis, at the beginning of polycytosis with normal protein concentration, but after ≈2 weeks, cytosis normalizes and the protein concentration increases). In tuberculosis, there is a very high concentration of protein.
TREATMENT AND PREVENTION to the top
As with encephalitis → section. 18.6.2 and meningitis →section. 18.6.1. Anti-inflammatory and decongestant treatment (dexamethasone) is of primary importance. In case of compression of the spinal cord by an epidural abscess → urgent surgical intervention (decompression).
Treatment
Treatment of this dangerous disease is carried out only in a hospital setting , it is long-term and complex, including drug therapy, physical therapy, careful care to prevent bedsores, massage and exercise therapy. Read more about some of these methods.
Drugs
Antibacterial drugs are prescribed for infectious inflammation of the spinal cord. In conservative treatment, antibacterial drugs are used to combat infection or septic complications . For this, Prednisolone is used, the course of treatment of which is 2-6 weeks, broad-spectrum antibiotics in large doses and sulfonamides.
They include desensitizing agents (Tavegil, Suprastin), vasodilators (Eufilin, Papaverine), hypocoagulants (Curantil, Heparin), antioxidants and vitamins C, group B, melliktin - to restore motor functions, reduce muscle tone in case of paralysis.
And if urination is impaired, they practice frequent catheterization , rinsing the bladder with manganese, boric acid, and prescribe diuretics and antimicrobial agents (Furagin, Furazolidone).
Bedsores are washed with peroxide, the pus is swabbed with sodium chloride, bandages with Vishnevsky ointment, syntomycin emulsion, sea buckthorn oil are applied to them, they are quartzed, and healing is accelerated by rinsing with insulin. To treat cystitis, chloramphenicol and biomycin are used.
Surgery
In the acute form of transverse myelitis with aggravating symptoms, treatment is only surgical. This method is also necessary for purulent or septic lesions located adjacent to the spinal cord .
Exercise therapy, massage
Passive exercise therapy classes are carried out from the second day of the disease.
Physical therapy exercises at different stages of the disease:
- In the first period they are done lying on the back, stomach or side, and possibly on all fours at a slow pace. ¾ of the complex consists of general strengthening and breathing exercises, and the rest is special. On days 10-15 they are supplemented with training of the buttocks, perineal and posterior muscles.
Exercise therapy for myelitis should be performed carefully and only under the supervision of a specialist. Then, lying on your stomach, train the muscles of the back and shoulder girdle 20-30 times. If the lower back and chest are affected, by the end of the month the patient should learn to roll over onto his stomach, then move in bed with the help of his hands, and within 2 months get on all fours (first with help). - In the second period, training of coordination, balance, stability while sitting and standing, maintaining posture in a calm state and when moving, predominates. This also includes exercises with a ball, a stick, against a wall, or on a walker. They are done 4-5 times a day with an instructor and independently.
- In the third period, maximum restoration of motor skills and body functions is achieved . These are a variety of activities with equipment and objects, games and dances. In the previous and especially this period, training in the pool (with fences, handrails and crossbars) is useful. For safety, the patient is wearing a cork belt.
To stimulate muscle tone and improve trophism and blood circulation, massage and electric massage of the muscles adjacent to the source of inflammation are useful. A dozen procedures are carried out for a quarter of an hour daily in several courses with three-week breaks.
Treatment at home
It is practiced during the recovery stage of the disease. At the same time, exercise therapy continues, folk remedies are used to relieve pain and minimize the destructive processes of the spinal cord. These are potato and honey cakes for the neck in the form of compresses. Compresses made from equal parts of aloe juice, dry mustard with the addition of vodka and propolis tincture are also useful; they are formed into a mass like plasticine and applied to the neck at night, covered with film.
Prevention
There is no specific prevention against myelitis; vaccination is practiced to prevent the disease. Prevention of infection is facilitated by timely treatment of chronic infections (sinusitis, caries, herpes) and complete cure of acute infectious diseases (influenza, measles).
Causes
There are often cases when the etiology of myelitis cannot be established. However, it is generally accepted that the main infectious agents that can provoke the development of myelitis are:
- Herpes virus;
- Cytomegalovirus infection;
- HIV;
- Mycoplasmas;
- Enteroviruses.
In addition, traumatic injury to the spinal cord and toxic-metabolic processes can be the root cause of myelitis.
Pathogenesis of myelitis
An infectious agent penetrating the spinal cord can primarily affect the white matter (leukomyelitis is formed) or the gray matter (poliomyelitis). First of all, swelling of the spinal cord occurs.
This condition contributes to circulatory disorders and changes the rheology of the blood. Thus, foci of ischemia are formed in the spinal cord, which are subsequently replaced by glial tissue.