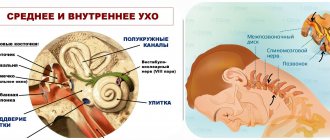
Vestibular disorder
The causes and mechanisms that cause dizziness in neurological diseases are not fully understood. Discussions continue to this day in medical scientific circles, and this despite the fact that in neurology, the most modern diagnostic methods are used to examine the structures of the brain and inner ear. Conventional drug therapy, which includes the use of sedatives, does not always have the desired effect, and in the case of long-term use, it can even have a negative impact on the processes of compensation of the functions of the vestibular system and the patient’s recovery. Vestibular disorders, manifested in vascular pathologies of the head, are the leaders among all vestibular manifestations known to medicine.
Dizziness: central and peripheral.
And so: what is dizziness?
Dizziness is a feeling of uncertainty in determining one’s position in space, apparent rotation of surrounding objects or one’s own body, a feeling of instability, loss of balance, the ground moving away from under one’s feet.
This is one of the most common reasons for visiting doctors of various specialties. Thus, in a survey of more than 20 thousand people aged 18 to 64 years, it turned out that more than 20% experienced dizziness in a month, of which more than 30% suffered from dizziness for more than 5 years. On average, about a quarter of the world's population suffers from vertigo.
The reasons for these sensations are different. At the same time, the scheme of differential diagnostic measures should cover a wide range of conditions, sometimes requiring the differentiation of such life-threatening conditions as acute cerebrovascular accident, cardiac arrhythmia and more common diseases of the inner ear, as well as dizziness of non-localized origin.
Various etiological factors include:
- diseases of the middle and inner ear of an inflammatory and non-inflammatory nature;
- diseases of the central nervous system;
- lesions of the neck organs, including degenerative-dystrophic changes in the cervical spine;
- metabolic and hematological causes;
- drug-induced disorders;
- infectious lesions;
- cardiogenic disorders;
- psychogenic disorders
- other reasons.
Classification of dizziness by etiology and clinical manifestations:
1.Vestibular or systemic:
— Peripheral:
- With hearing impairments;
- No hearing impairment.
-Central;
- Non-vestibular or non-systemic;
Most often, vestibular (systemic) spinning in the head occurs against the background of pathologies of the vestibular, visual apparatus or musculoskeletal system.
Peripheral vestibular vertigo occurs when the sensory elements of the ampullary apparatus and vestibule, vestibular ganglion and nerve conductors of the brain stem are damaged and is characterized by a paroxysmal course, variable intensity, accompanied by ataxia and autonomic manifestations. With an acute onset, patients feel the movement of objects towards a more actively working labyrinth; nystagmus is also directed in the same direction - spontaneous regular, clonic, horizontal or horizontal-rotatory nystagmus, of varying intensity and degree, associated with a harmonious deviation of the torso and arms towards the slow component . There is a positive effect of changing the position of the head (towards the slow component of nystagmus). As a rule, peripheral vestibular vertigo is a one-sided process and is accompanied by impaired auditory function on the affected side, however, in a number of diseases that most clearly reflect the true clinical picture of peripheral vestibular syndrome (benign paroxysmal positional vertigo, vestibular neuronitis and, for the first time, in the vestibular form of Meniere's disease) , hearing remains intact.
- Benign paroxysmal positional vertigo (BPPV) is the most common type of otogenic vertigo, occurring in approximately 20% of all cases of vertigo and 50% of cases of otogenic vertigo. The clinical picture of BPPV is characterized by short episodes of dizziness, provoked by changes in head position. BPPV is caused by otolith debris in the posterior canal of the inner ear. dizziness in a patient
- Vestibular neuritis is characterized by dizziness, nausea, ataxia and nystagmus. The clinical picture of labyrinthitis is represented by the same symptom complex in combination with tinnitus and/or hearing loss. Vestibular neuritis and labyrinthitis are the causes of dizziness of otogenic origin in 15% of cases.
- The clinical picture of Meniere's disease is characterized by periodic dizziness, accompanied by hearing impairment. In Meniere's disease, expansion and periodic rupture of the endolymphatic receptacle of the inner ear is observed. Meniere's disease affects approximately 15% of patients with otogenic vertigo.
- Bilateral vestibular paresis is manifested by oscillopsia and ataxia. It is usually caused by a decrease in the number of vestibular hair cells. Typically, previous use of ototoxic antibiotics (intravenous or intraperitoneal) for several weeks, most often gentamicin. Bilateral vestibular loss is uncommon.
- Perilymphatic fistula (PS) is manifested by sensitivity to changes in pressure or hydrops symptom complex, or ataxia caused by physical activity. In PS, there is communication between the fluid-filled inner ear and the air-filled middle ear. Barotrauma, such as from scuba diving, is the most common mechanism of PS. Another common cause of PS is surgery to treat otosclerosis or cholesteatoma. PS is extremely rare.
- The clinical picture of tumors compressing the eighth cranial nerve is characterized by asymmetric hearing impairment, accompanied by moderate ataxia. Among patients suffering from vertigo, tumors of the eighth cranial nerve are rare; they are more often observed in cases of unilateral hearing loss.
Central vestibular vertigo
Its cause is dysfunction of the central structures that ensure the conduction of sensitive impulses from the inner ear, their connection with the vestibular nuclei in the brain stem, with the cerebellum, with the oculomotor nuclei, as well as communication with the cerebral cortex. This type of lesion is characterized by a sensation of pushing forward, backward, to the sides, and the presence of other signs of central nervous system damage: diplopia, dysarthria, loss of sensitivity, paresis.
The most common signs of central damage to the vestibular system are
- vertical nystagmus;
- nystagmus changing direction;
- atypical nystagmus (especially downward nystagmus) in the head shake test;
- asymmetric oculomotor dysfunction;
- severe postural instability with falls.
In most cases, central vertigo is caused by vascular disorders (stroke, transient ischemic attack, vertebrobasilar migraine), which accounts for 60% of calls.
- Stroke and transient ischemic attack (TIA), in which pathological changes occur in the brain stem or cerebellum, cause central vertigo in approximately 1/3 of cases. Isolated dizziness can sometimes be the only symptom preceding a stroke localized in the structures of the posterior cranial fossa. Almost always, symptoms of dizziness are accompanied by other focal signs of central nervous system damage.
- Vertebrobasilar migraine most often presents with dizziness and headache, but may present as dizziness alone. Migraine causes about 15% of all cases of central vertigo. Migraines are especially common in women between the ages of 30 and 40. The attacks are stereotypical, often accompanied by photophobia, soundphobia, visual or other aura.
- Epileptic seizures are characterized by dizziness combined with confusion, motor symptoms, or, more commonly, a spinning sensation. About 5% of cases of central vertigo are associated with epileptic seizures.
- In multiple sclerosis (MS), dizziness is combined with other signs of central nervous system damage, for example, cerebellar dysfunction. MS is not a common cause of dizziness, although many patients consider this disease to be the cause of such symptoms. The share of PC in the structure of all cases of central vertigo is 2%.
- Arnold-Chiari malformation is a developmental anomaly in which there is a hernial protrusion of the cerebellar tonsils 5 mm or more below the level of the foramen magnum. Patients complain of dizziness, ataxia and headaches in the occipital region; they often experience vertical nystagmus. Symptoms are triggered by straining and coughing. Occurrence: 1% of all cases of central vertigo.
Non-vestibular (non-systemic) dizziness is a feeling of lightheadedness, loss of stability, loss of balance, “loss of ground under your feet,” “darkening in the eyes,” and ringing in the ears. Often, these conditions precede the development of fainting (lipothymia), although complete loss of consciousness may not occur. Characteristic of states of non-systemic dizziness are pronounced emotional disorders - a feeling of restlessness, anxiety, fear or, conversely, depression, powerlessness, a sharp loss of strength. A number of patients experience a combination of manifestations of both systemic and non-systemic dizziness. Especially often, a similar picture occurs in elderly and senile patients, against the background of a combination of several predisposing factors.
Causes of mixed and non-systemic dizziness of non-cerebral origin include fluctuations in blood pressure, low blood sugar and/or metabolic disorders associated with medications or systemic infection. In most cases, these conditions require emergency care and are observed in 33% of patients with attacks of dizziness. Such conditions are rare when seen by specialists (2-5%). Basically, these are conditions that a doctor may encounter during emergency care.
- Postural hypotension may cause lightheadedness, weakness, blurred vision, or fainting. This condition is observed only when the patient is in an upright position.
- The clinical picture of cardiac arrhythmia is characterized by fainting or a sudden fall. As with postural hypotension, clinical symptoms develop only when the patient is in an upright position.
- Hypoglycemia and metabolic disorders are manifested by weakness, lightheadedness, dizziness, and darkening of the eyes. Taken together, they account for about 5% of cases among patients with non-systemic dizziness of non-cerebral origin.
- When exposed to drugs or other substances, weakness, lightheadedness, and darkening of the eyes usually occur, but true dizziness can also develop. This condition is diagnosed in 16% of patients with all types of dizziness during emergency care, but is rare outside the emergency department. Most often, such disorders are caused by antihypertensive drugs, especially alpha-adrenergic blockers, for example, terazosin, calcium channel blockers with a pronounced vasodilating effect, for example, nifedipine, and sedatives. Some commonly prescribed benzodiazepines, such as Xanax, cause dizziness, which is part of the drug's withdrawal symptoms. Drugs that suppress vestibular dysfunction, such as meclizine and scopolamine, may cause these sensations by acting directly on the central vestibular pathways.
- Viral infections that are not accompanied by ear damage, according to the literature, can cause a symptom complex of dizziness in 4-40% of patients who seek emergency help for this reason. Clinical manifestations of viral infections may include, for example, gastroenteritis and flu-like symptoms.
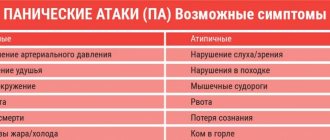
- Psychogenic dizziness is obligately accompanied by severe fear and anxiety, as well as autonomic disorders - cardiovascular and respiratory. Most often, dizziness is observed against the background of hyperventilation syndrome; rapid and shallow breathing leads to metabolic disorders, increased neuromuscular excitability, etc. In this case, patients define their sensations as lightheadedness, lightness of the head, and often the symptoms of dizziness are combined with noise and ringing in the ears, increased sensitivity to sound stimuli, instability when walking. Psychogenic dizziness often occurs during a panic attack . Symptoms of fear, shortness of breath, palpitations, and nausea may occur simultaneously with symptoms of lightheadedness, lightheadedness, fear of falling, and loss of balance.
There are more than 80 diseases, one of the symptoms of which is dizziness. To understand which of them caused systemic dizziness, you should consult a therapist. After a thorough examination, questioning and history taking, he can make a diagnosis. If the cause cannot be identified, additional diagnostic methods are prescribed: CBC, LBC, CT/MRI of the brain, cervical spine, EEG, LA, ultrasound of the central nervous system, ECG/Holter ECG, examinations by various specialists: ENT doctor, neurologist, cardiologist and etc. as needed.
The specialist doctor performs simple diagnostic techniques that do not require special equipment, allowing for a differential diagnosis of dizziness: the de Klein test, the Dix-Hallpike test, the Halmage test (head rotation test) and the head shaking test and other techniques.
Treatment : the main groups of basic therapy drugs used in the treatment of dizziness:
- Antihistamines (Clemastine, meclozine (25-100 mg/day in the form of chewable tablets) improve the general condition of the patient in the first 2-3 days of the disease.
- Angioprotector-vertigolytic betahistine 24 mg 2 times a day (48 mg per day) helps restore balance for 2-3 months or more
- Vasoregulatory drugs (Vinpocetine, Nicergoline).
- Nootropics (Piracetam, Nootropil, Phenibut, choline alfoscerate, etc.).
- Tranquilizers (diazepam 10 mg (2.0) IM and others). They are able to eliminate anxiety and panic attacks. The use of drugs that have a sedative effect is possible in the first 2-3 days of acute dizziness
- Eufillin and Metoclopramide will help with nausea and vomiting. The use of dimenhydrinate (50-100 mg 2-3 times a day), diphenhydramine (25-50 mg orally 3-4 times a day or 10-50 mg intramuscularly) is also recommended.
- Vestibular gymnastics.
Depending on the immediate cause of the disease, additional etiotropic, pathogenetic, metabolic and prophylactic drugs are used.
Relief of acute vestibular syndrome involves the use of antiemetics (antiemetics) and vestibular suppressants. The duration of use of vestibular suppressants and antiemetics is limited by their ability to slow down vestibular compensation and should not exceed 2-3 days.
In case of vestibular neuronitis and labyrinthitis, intramuscular administration of vestibular suppressants and antiemetics is indicated in the first 2–3 days to relieve the manifestations of acute vestibular crisis. After nausea has stopped for 1–3 months, betahistine is prescribed orally at a daily dose of 48 mg. During the same period, a course of vestibular rehabilitation (gymnastics) should begin according to an individual program. Depending on the characteristics of the pathogenesis of vestibular neuronitis and labyrinthitis, appropriate drug treatment is prescribed. Thus, for vestibular neuronitis, relatively high doses of glucocorticosteroids are used, for example, methylprednisolone at an initial dose of 100 mg, followed by a dose reduction of 20 mg every 3 days. Treatment of labyrinthitis may require antibacterial or antiviral drugs, depending on the pathogen. In addition, for labyrinthitis, in some cases surgical treatment is resorted to. With labyrinthitis, unlike vestibular neuronitis, patients often require subsequent auditory rehabilitation.
The use of drug treatment for BPPV . The Semont and Eple maneuvers (methods) and the Brandt-Daroff exercises are considered preferable and most popular for the treatment of BPPV in cases of damage to the posterior canal.
For an acute fistula, conservative treatment is quite effective with mandatory bed rest for a week (the head should be elevated) and the exclusion of physical activity for another 1.5–2 months.
For Meniere's disease, in the interictal period, complex treatment (maintenance therapy) is indicated to prevent the development or reduce endolymphatic hydrops: diuretics, vasodilators (histamine analogue-betagistine in a daily dose of 48 mg for 2-3 months or more), corticosteroids.
Planned (preventive) treatment of vestibular migraine is carried out in accordance with the classical principles of migraine treatment using beta blockers, anticonvulsants, tricyclic antidepressants and selective serotonin and norepinephrine uptake inhibitors.
Treatment of central vertigo associated with stroke at VBB is carried out according to the principles of stroke therapy in a neurological hospital for stroke patients.
Surgical treatment of vertigo is applicable to space-occupying lesions and abnormalities.
In some particularly severe cases, surgical treatment for peripheral vertigo is possible. In case of BPPV, filling of the affected semicircular canal with bone chips is indicated in case of ineffectiveness of therapeutic maneuvers (0.5-2% of BPPV cases).
If conservative treatment is ineffective for other causes of peripheral vestibular vertigo, the following may be performed:
- Selective neurectomy of the vestibular nerves;
- Labyrinthectomies;
- Laser destruction of the labyrinth.
It is recommended to carry out vestibular rehabilitation . Correction of the patient's anxiety, feelings of uncertainty and fear is mandatory. Preference should be given to vestibular rehabilitation using special installations - postulographic and stabilographic complexes, which allow simultaneous assessment of the effectiveness of treatment. An active rehabilitation strategy with early activation of the patient is necessary.
specific prevention of peripheral dizziness.
Department of Neurology, 10th City Clinical Hospital
neurologist Drik O.N.
What diseases cause vestibular disorders?
Vestibular disorders have the following causes:
1. People aged 60 years and older often experience benign positional vertigo, which occurs against the background of traumatic brain injury, otitis media, and ischemia. However, there are cases where the exact reasons were not established.
This vestibular disorder is characterized by the following symptoms and external signs: a person changes his body position in bed (lays down, stands up, turns around), and he experiences a short-term attack of dizziness. In most patients, the exacerbation phase (attacks of dizziness occur quite often) is replaced by a spontaneous long-term remission.
To confirm the diagnosis, special so-called positional tests are used - the person changes the position of the head, and doctors record when nystagmus and dizziness occur.
The appearance of this disease is facilitated by the formation of otoliths in the posterior semicircular canal. The force of gravity acts on the otoliths, and they shift, irritating the vestibular receptors of the dome, which leads to dizziness. This condition can last for a very long time without the manifestation of any other disorders.
Treatment of this vestibular disorder with traditional medications often does not produce the desired effect. In cases where the body is particularly resistant to certain medications, surgical intervention is indicated. Severe outbreaks of positional vertigo have another cause - the loop of the anterior inferior cerebellar artery compresses the vestibular nerve, which leads to decreased hearing sensitivity, tinnitus and hyperacusis. Taking carbamazepine (finlepsin) usually helps to relieve the manifestations of this disease, and in cases of ineffectiveness of the drug, a procedure such as microvascular decompression of the nerve is used. Drinking alcohol leads to changes in endolymph density, and this can also cause dizziness.
2. Another fairly well-known cause of dizziness is vestibular neuritis. It is caused by damage to the vestibular nerve or peripheral vestibular apparatus. People of all ages are susceptible to the disease. It is often preceded by infectious diseases affecting the upper respiratory tract. In this case, the following symptoms of the disease and its external signs are distinguished: sudden rotational movements of the head cause an attack of dizziness, vomiting, and a feeling of nausea. The presence of horizontal rotatory nystagmus is observed. An important fact is that in the case of this disease, the nystagmus has only a unilateral direction, while in the case of a bilateral one, we are talking about a different diagnosis. Vestibular neuritis is characterized by the absence of other neurological symptoms (for example, decreased hearing sensitivity). Attacks of severe dizziness, accompanied by repeated vomiting, last in the patient for 3-4 days, but complete remission occurs only after a few weeks. In cases where the patient’s condition does not improve within a month, he is sent to magnetic resonance or computed tomography for additional research. Mild cases of the disease do not require hospitalization; outpatient treatment is quite possible. At the initial stage, short-term treatment with corticosteroids is often prescribed - they reduce vestibular symptoms. The positive effect and improvement in the patient’s condition provide grounds for discontinuing medications and prescribing special exercises to strengthen the vestibular apparatus.
3. The root cause of vestibular disorders in older people with a history of vascular diseases is often vertebrobasilar insufficiency. It can be caused by pathologies such as ischemia of the labyrinth or vestibular nerve or trunk. This vestibular disorder is characterized by the acute development of an attack of dizziness, the presence of disturbances in the functioning of the vestibular system, vomiting, and a feeling of nausea. In some cases of ischemia of adjacent sections of the trunk, other external signs are observed - a person may suddenly fall, he is disoriented, his vision is impaired, his limbs become flaccid and numb.
The occurrence of vertebrobasilar insufficiency can also be caused by some other reasons: atherosclerosis of the arteries, sometimes cardiogenic embolism, increased blood viscosity, vasculitis. To accurately diagnose this disease, it is necessary to take into account the symptoms of various concomitant diseases in the medical history, namely arterial hypertension (high blood pressure), diabetes mellitus, hyperlipidemia. The entire course of treatment for vertebrobasilar insufficiency is primarily aimed at correcting or eliminating risk factors, and includes taking antiplatelet and vasoactive drugs.
4. Blockage of the internal auditory artery is one of the most persistent types of vertigo. The most common external sign of this disease is hearing loss. Cerebellar ataxia and nystagmus, coupled with an acute attack of dizziness, may indicate hemorrhage or cerebellar infarction. And in these cases, emergency intervention is required, since we are talking about human life and death. The initial stage of cerebellar stroke is very similar to vestibular neuritis. And they differ in nystagmus, which in this disorder is bilateral or vertical. The patient is also unable to stand without assistance.
5. Slowly increasing imbalance and moderate dizziness indicate chronic bilateral vestibulopathy. The cause of the disease can be intoxication of the body with certain types of medications. Timely discontinuation of the medication helps restore vestibular function. If this is not done in time, the process becomes irreversible. Various types of solvents, chemicals, and loop diuretins can also sometimes cause a vestibular disorder called chronic vestibulopathy.
6. Here are the known symptoms of Meniere's Disease: dizziness that occurs occasionally, congestion and tinnitus, accompanied by a decrease in hearing sensitivity. An acute attack of dizziness reaches its maximum in a few minutes and regresses in the following hours. At the very beginning of the disease, the process of hearing loss can be stopped. But each subsequent attack leads to the fact that hearing sensitivity becomes lower and lower. In this case, constant tinnitus appears, which intensifies before the onset of an attack and during it. Some patients may fall suddenly without losing consciousness. The reason for this is a sharp increase in pressure in the inner ear and, as a result, irritation of the vestibular receptors. In the process of diagnosing this vestibular disorder, the main condition is the exclusion of other diseases, for example, SLE, neurosyphilis or hypothyroidism.
7. Injuries to the skull and head can often become a source of post-traumatic vertigo. This occurs due to concussion of the labyrinth, the formation of a perilymphatic fistula, or a violation of the integrity of the temporal bone.
8. There are a number of other ear diseases that can cause vestibular disorders. These include: common wax plugs in the ears, Eustachian tube dysfunction, otosclerosis. Otitis media in acute form can also cause dizziness, especially if it is complicated by purulent processes in the labyrinth.
9. One of the rather rare and infrequent causes of dizziness is a tumor of the cerebellopontine angle. A gradual and slow process of hearing loss, as well as constant tinnitus, indicate a disease such as acoustic neuroma.
10. Let us note another cause of vestibular disorders - basilar migraine. Girls in the prepubertal period are most susceptible to migraine dizziness and pain. They last no more than an hour and are relieved by taking anti-migraine medications.
11. Short-term attacks of dizziness can also occur with epilepsy. But along with them, other symptoms of an epileptic seizure are usually observed: motor, autonomic or sensory, and a disturbance of consciousness is necessarily present.
12. Craniovertebral anomaly - we are talking about it when attacks of dizziness are combined with nystagmus and impaired speech and swallowing functions. Symptoms such as vomiting, nausea, dizziness with rotational movements of the head can signal the initial stage of multiple sclerosis.
Damage to the posterior semicircular tubule
The Dix-Hallpike test is the “gold standard” for diagnosing BPPV caused by posterior SCC pathology:
- The patient sits straight along the couch, with his head turned 45˚ towards the labyrinth that is being examined.
- The patient is placed in a lying position, while the head rotation is maintained, the head is thrown back at an angle of 30˚ relative to the axis of the body, and hangs over the edge of the couch.
- Watch eye movements. Nystagmus and dizziness occur with a delay of several seconds and last less than 1 minute. Nystagmus has a typical trajectory: first, a tonic phase occurs, during which the eyeball is moved upward, away from the underlying ear, a rotatory component is noted, then clonic eye movements toward the floor occur. the underlying ear.
- After the nystagmus stops, the patient is returned to a sitting position and the eye movements are observed again; the nystagmus may reappear, but in the opposite direction.
When the test is repeated with turning the head in the same direction, the intensity and duration of the nystagmus decrease each time.
The procedure is repeated with the head turned in the opposite direction.
The affected side is determined by which side positional nystagmus and dizziness occur.
Which doctors should I contact if a vestibular disorder occurs?
If you notice disturbances in your vestibular state, you should definitely seek advice from a specialist - a neurologist. Based on certain symptoms and external signs, only a doctor can make an accurate diagnosis. Therefore, if you find signs of a neurological disease, seek help from a neurologist. Do not put your health at risk - do not self-medicate.
Primary appointment with a neurologist: 1850 RUR.
Sign up Online 5% discount when registering from the site
Read also
Sulfur plug
What is a cerumen plug? Inside the ear canals there are glands that secrete a special secretion - sulfur.
This is a rather thick and sticky substance that protects the ear from dirt and dust. Ideally, it should... Read more
Hoarseness of voice
What is Hoarseness Hoarseness is an abnormal change in voice that is a common symptom that often occurs in combination with a dry or scratchy throat. If your voice is hoarse...
More details
Benign positional paroxysmal vertigo
How great it is when you feel dizzy with happiness, but unfortunately there are people who are afraid of this symptom because this symptom greatly interferes with their quality of life. Dizziness is not a diagnosis, it is a symptom...
More details
Adenoids
Probably, in modern times there is not a single parent who has not heard at least once about adenoids. This is the first question that is asked at an appointment with an ENT doctor: “Do we have adenoids?” What are adenoids?...
More details
Ear congestion
Sometimes people take the health of their hearing organs lightly and begin to take action only in case of severe discomfort, ignoring such a problem as ear congestion. So that you don’t have to overcome it in the future...
More details