Classification of jaw atrophy and bone tissue phenotypes
Depending on the position of the jaw, there are two groups that characterize the atrophic state of the upper and lower jaws:
- According to Schroeder for the top row. There are three types of upper jaws with missing teeth, resulting in thinning bone tissue:
- The jaw tubercles are very noticeable. These gaps can be filled with prosthetic implants because the physical abnormalities are not noticeable. The palate is deep, and the bend of the mucosa is quite large.
- The alveolar processes are not clearly defined. The depth of the sky is average. Prosthetics are possible, but their fixation may deteriorate after muscle tissue overstrain.
- The bone at the base of the jaw is seriously destroyed. The ridges and tubercles of the alveoli are smooth, and the palate is transformed into a flat shape. The fold of the mucous membrane becomes at the level of the palate and does not hold its shape well. As a result of pathology, prosthetic structures cannot be secured.
- According to Keller for the bottom row:
- The alveolar elements are slightly smoothed, but are visible throughout the entire jaw. At the beginning of the alveolar ridge, muscle tissue and a fold of mucous membrane are attached. Installation of the prosthesis is not difficult.
- The ridge becomes noticeable and takes on a sharper shape. The muscles are attached to the crest. In most cases, the implant causes discomfort and pain.
- It is often observed in people who have undergone early removal of lateral teeth. The alveoli around the molars and premolars become thinner. In the central part, the bone tissue does not lose volume. Creating artificial teeth is possible, but there is a possibility of the implant slipping when chewing.
- In the area of the frontal incisors, a pronounced atrophic process is observed, while the lateral dentition remains preserved. Fixation of the prosthesis cannot be done, because the likelihood of its displacement increases.
Symptoms of atrophy
The patient is concerned about decreased visual acuity, which is not amenable to optical correction.
In this case, visual disturbances can manifest themselves in the form of separate “spots” before the eyes or a sensation of narrowing of the fields up to “tubular vision”. Color vision disturbances are also possible.
The dynamics of symptoms may vary. Sometimes atrophy progresses steadily without treatment, even to the point of blindness. Also, the atrophic process can be suspended. In this case, the decrease in vision can be significant, but complete blindness does not develop.
Implantation for jaw bone atrophy
Several techniques are used to quickly restore the dentition. For example, installation of bridges or removable dentures. However, these methods cannot restore the required load on the bone, since the gums or healthy teeth are loaded.
Implantation helps relieve pressure on the bone and prevent further thinning.
In advanced cases, when the atrophy of the jaw bone tissue is significant, restoration of the bone structure is used before implantation. Various techniques are used, for example, sinus lifting, separation of the alveolar process, and the introduction of artificial tissue. Six months after the operation, implants are inserted. As a result, bone density and volume are preserved.
Implantation with immediate loading is considered a new technique. Special materials are installed not in the alveolar process, but in the basal part of the jaw. Thanks to this, the bone is immediately loaded, and the metabolism is not disrupted. Suitable only if three or more teeth in a row are missing.
Diagnostics
The diagnosis of retinal atrophy can be made after examining the fundus. The disease is characterized by very specific signs: increased pigmentation of the macula, scattered or merging atrophic foci on the retina in the dry form of the disease, or swelling of the retina with increased vascular pattern in the wet form. The patient’s subjective complaints also help determine the diagnosis.
To confirm the diagnosis, instrumental methods are used:
- biomicroscopy of the eye, during which the doctor examines the internal structures of the organs of vision through a special slit lamp under multiple magnification;
- visometry - measurement of visual acuity using special tables: the patient looks alternately with both eyes and names the images that the doctor points to;
- angiography - radiographic examination of the blood vessels of the eyes with contrast;
- Ultrasound scanning with Dopplerography, revealing vascular obstruction;
- CT scan of the eyes, determining the boundaries of retinal ischemia and atrophy.
If vascular anomalies are detected, additional tests may be prescribed: blood tests for glucose and cholesterol, general clinical laboratory tests of blood and urine, etc. An ophthalmologist writes out referrals for examinations. In the future, doctors of other specializations may be involved: therapists, surgeons, phlebologists and cardiologists.
Types and degrees of jaw bone atrophy
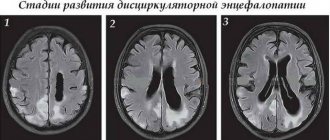
Deformation of the jaw bone develops with different intensity:
- I degree. At the beginning of the disease, it is eliminated by prosthetics. The implant performs its function, the blood supply is not disrupted.
- II degree. The clinical picture is intensifying. The mucous membrane of the jaw begins to shrink. Dental prosthetics are possible, but additional treatment is required before this can be done.
- III degree. The contour of the bone tissue is smoothed both on the inside of the mouth and on the side of the chin.
When selecting a treatment method, this characteristic of the development of pathology should be taken into account. Bone tissue decreases not only in height, but also in width. The bone becomes short and thin.
Jaw bone atrophy with age
One of the factors influencing the defect is age-related changes. As a rule, in patients over 60 years of age, atrophy is a common process. This is explained by the fact that the lack of minerals and cell nutrition affects metabolism and teeth fall out. The blood supply to bone tissue is disrupted and the required amount of oxygen is not supplied. This causes a change in pressure on the bone.
Adaptation
Adaptation in pathology can reflect various functional states: functional tension, decrease or distortion of tissue (organ) function. In this regard, it can manifest itself in various pathological processes:
- atrophy;
- hypertrophy (hyperplasia);
- organization;
- tissue restructuring;
- metaplasia;
- dysplasia.
1. Atrophy (a - exception, Greek trophe - nutrition) - intravital decrease in the volume of cells, tissues, organs - is accompanied by a decrease or cessation of their function.
Not every organ reduction is related to atrophy. Due to disturbances during ontogenesis, the organ may be completely absent - agenesis, retain the appearance of an early rudiment - aplasia, or not achieve full development - hypoplasia. If there is a decrease in all organs and a general underdevelopment of all body systems, they speak of dwarfism.
Atrophy is divided into physiological and pathological.
Physiological atrophy is observed throughout a person’s life. Thus, after birth, the umbilical arteries and the ductus arteriosus become atrophied and obliterated; in older people, the gonads atrophy; in old people, bones, intervertebral cartilage, etc.
Pathological atrophy is caused by various reasons, among which the most important are malnutrition, impaired blood circulation and activity of the endocrine glands, the central and peripheral nervous system, and intoxication. Pathological atrophy is a reversible process. After removing the causes of atrophy, if it has not reached a high degree, complete restoration of the structure and function of the organ is possible.
Pathological atrophy can be general or local in nature.
General atrophy, or exhaustion, occurs in the form of nutritional exhaustion (during starvation or impaired absorption of food); exhaustion due to cancer cachexia (from the Greek kakos - bad, hexis - condition); exhaustion due to pituitary cachexia (Simmonds disease with damage to the pituitary gland); exhaustion due to cerebral cachexia (damage to the hypothalamus); exhaustion due to other diseases (chronic infections such as tuberculosis, brucellosis, chronic dysentery, etc.).
The appearance of patients with exhaustion is characteristic. There is a sharp loss of weight, subcutaneous fatty tissue is absent; where it is preserved, it has a brownish color (accumulation of lipochrome pigment). The muscles are atrophic, the skin is dry and flabby. Internal organs are reduced in size. Brown atrophy (accumulation of lipofuscin pigment in cells) is observed in the liver and myocardium. In the endocrine glands there are atrophic and dystrophic changes, expressed to varying degrees depending on the cause of depletion. Areas of dead nerve cells are found in the cerebral cortex. Osteoporosis develops.
Local atrophy occurs from various reasons. The following types are distinguished: dysfunctional; caused by insufficient blood supply.
Dysfunctional atrophy (atrophy from inactivity) develops as a result of decreased organ function. This is muscle atrophy due to bone fractures, joint diseases that limit movement; optic nerve after eye removal; edges of a toothless cell. The metabolic rate in the tissues is reduced, and an insufficient amount of blood and nutrients flows to them.
Atrophycaused by insufficient blood supply, develops due to narrowing of the arteries supplying this organ. Insufficient blood flow causes hypoxia, as a result of which the activity of parenchymal elements decreases and cell size decreases. Hypoxia stimulates fibroblast proliferation and sclerosis develops. This process is observed in the myocardium when cardiomyocyte atrophy and diffuse cardiosclerosis develop due to progressive atherosclerosis of the coronary arteries; With sclerosis of the renal vessels, atrophy and wrinkling of the kidneys develop.
atrophy develops even in organs consisting of dense tissue. With prolonged pressure, violations of tissue integrity (usures) occur, for example in the vertebral bodies, in the sternum with the pressure of an aneurysm. Pressure atrophy occurs in the kidneys when the outflow of urine is obstructed. Urine stretches the lumen of the pelvis, compresses the kidney tissue, which turns into a bag with thin walls, which is referred to as hydronephrosis. When the outflow of cerebrospinal fluid is obstructed, the ventricles expand and brain tissue atrophies (hydrocephalus). Pressure atrophy is based essentially on insufficient blood flow to the cells and the resulting hypoxia.
Neurotic atrophy is caused by disruptions in the connection between the organ and the nervous system, which occurs when nerve conductors are destroyed. Most often, this type of atrophy develops in striated muscles as a result of the death of motor neurons of the anterior horns of the spinal cord or nerve trunks related to these muscles (with poliomyelitis, with inflammation of the facial nerve).
Striated muscles atrophy unevenly, while intermuscular connective and adipose tissue grows rapidly. In this case, the tissue mass may increase (false hypertrophy).
Atrophy under the influence of physical and chemical factors is a common occurrence. Under the influence of radiation energy, atrophy is especially pronounced in the bone marrow and genitals. Iodine and thiouracil suppress the function of the thyroid gland, which leads to its atrophy. With long-term use of ACTH and corticosteroids, atrophy of the adrenal cortex may occur and adrenal insufficiency may develop.
A peculiar type of adaptive atrophy is acute involution of the thymus
The appearance of the organ with local atrophy is different. In most cases, the size of the organ decreases, its surface is smooth (smooth atrophy). Less commonly, organs, such as the kidneys and liver, take on a granular or lumpy appearance (granular atrophy). With hydronephrosis, hydrocephalus, false hypertrophy, the organs are enlarged, but not due to parenchymal elements, but due to the accumulation of fluid or the proliferation of fatty tissue. Sometimes this fiber grows around an atrophied organ, such as a kidney.
The significance of atrophy for the body is determined by the degree of reduction of the organ and decrease in its function. If atrophy and sclerosis have not reached a large degree, then after eliminating the cause that caused the atrophy, restoration of structure and function is possible, as mentioned earlier. Under certain conditions, an atrophied organ may subsequently even undergo hypertrophy. Far advanced atrophic changes are irreversible.
In experiments on rats, for example, it was established that with stenosis of the arteries of one of the kidneys, atrophy of the corresponding kidney occurs, but if after this the lumen of the artery of the contralateral kidney is further narrowed, then the kidney that previously underwent atrophy hypertrophies.
Hypertrophy (hyperplasia). Hypertrophy (from the Greek hyper - excessively, trophe - nutrition) can be adaptive in nature - an increase in the volume of a cell, tissue, organ due to cell proliferation or an increase in the number and size of intracellular ultrastructures. Two types of hypertrophy are considered adaptive: neurohumoral hypertrophy (hyperplasia) and hypertrophic growths.
Neurohumoral hypertrophy and hyperplasia occur due to dysfunction of the endocrine glands (hormonal or correlative hypertrophy and hyperplasia). The physiological prototype of such hypertrophy and hyperplasia, which undoubtedly has an adaptive significance, can serve as hypertrophy of the uterus and mammary glands during pregnancy and lactation. In conditions where ovarian dysfunction occurs, gland hyperplasia develops in the uterine mucosa, sometimes with cystic expansion of their lumen - the so-called glandular-cystic endometrial hyperplasia, accompanied by irregular uterine bleeding. During atrophic processes in the testicles, hyperplasia of the glandular lobules develops in the mammary gland of men, which leads to an increase in the size of the entire gland - gynecomastia is noted (from the Greek gyne - woman, matos - breast). Hyperfunction of the anterior lobe of the pituitary gland, which usually occurs due to adenoma, is accompanied by an increase in organs and protruding parts of the skeleton - acromegaly develops (from the Greek akros - extreme, protruding, megalos - large). Correlative hypertrophies and hyperplasias, which arise as a reaction to certain hormonal stimuli, are often the basis for the tumor process.
Hypertrophic growths , leading to an increase in the size of tissues and organs, occur as a result of various reasons. They often occur with chronic inflammation (for example, on the mucous membranes with the formation of polyps), with impaired lymph circulation in the lower extremities and lymph stagnation, which leads to the proliferation of connective tissue (development of elephantiasis). Hypertrophic proliferation of adipose and connective tissue occurs with partial or complete atrophy of an organ (false hypertrophy). Thus, with muscle atrophy, adipose tissue grows between their fibers; with kidney atrophy, the growth of adipose tissue around it increases; with brain atrophy, the bones of the skull thicken; When the pressure in the vessels decreases, their intima grows.
All of the listed processes of hypertrophic growth of supporting tissue filling the space occupied by an organ or tissue are called vacate (from the Latin vacuum - empty) hypertrophy.
Organization. An organization that is one of the manifestations of adaptation is the replacement of an area of necrosis or thrombus with connective tissue, as well as encapsulation.
Jaw bone atrophy after tooth extraction
The most common cause of the disease is the loss of a tooth or dentition. A few months after extraction, if prosthetics are untimely, the process of reducing the jawbone begins due to pressure on the alveolar process. Within a year, the deformation can reach its maximum.
The consequences of bone tissue deficiency are expressed in the deterioration of speech, changes in the proportions of the face and its shape, and the appearance of severe wrinkles in the mouth area. At an advanced stage, patients experience displacement of the dentition, loss of opposite and/or adjacent teeth. Because of this, the likelihood of implantation failure increases.
Optic nerve atrophy - symptoms and treatment
Optic atrophy is the thinning and destruction of the nerve fibers of the optic nerve, a decrease in the number of retinal ganglion cells that generate nerve impulses and transmit them from the eye to the brain. Damage to nerve fibers occurs as a result of their inflammation, swelling, compression, circulatory disorders, damage and replacement with connective tissue.
In the International Classification of Diseases (ICD-10), optic atrophy is listed under code H47.2.
Often this pathology is a symptom of other ophthalmological, neurological and systemic diseases. It is accompanied by deterioration of vision and can lead to irreversible blindness.
Cause of congenital optic atrophy
Optic atrophy occurs in both children and adults. In children, this disease is most often congenital. It is formed as a result of genetic disorders, birth trauma, previous inflammatory or congenital oncological diseases.
Causes of acquired optic atrophy
In adults, atrophy usually develops as a result of vascular, inflammatory or degenerative disorders in the optic nerve [1][3][6].
There are many reasons for the development of atrophy. The main ophthalmological causes include:
- diseases associated with inflammation of the optic nerve: intrabulbar and retrobulbar neuritis (inflammation of the optic nerve within and behind the eyeball);
- acute and chronic diseases of the optic nerve, in which blood flow in the vessels supplying the nerve is reduced: diabetic retinopathy, retinal edema and angiopathy, ischemic optic neuropathy, retinal vein thrombosis, etc.;
- congestive optic disc is swelling of the optic disc associated not with inflammation, but with increased intracranial pressure. The causes of the development of a stagnant disc can be brain diseases: hemorrhages, tumors, abscesses, meningitis, thrombosis, traumatic brain injuries;
- orbital diseases: intraocular tumors, abscesses;
- glaucoma;
- retinal degeneration.
Traumatic causes of atrophy are various injuries to the skull as a result of a car accident, domestic incidents, or a gunshot wound. They are accompanied by contusion, compression, separation or rupture of the optic nerve.
Also, atrophy of the optic nerve develops with toxic lesions : acute and chronic poisoning with methyl or ethyl alcohol, tobacco, quinine, pesticides, drugs (amiodarone, barbiturates, sulfonamides, etc.).
The causes of congenital optic atrophy include intrauterine poisoning, inflammatory diseases of the mother during pregnancy, improper management of pregnancy and childbirth, birth injuries, and developmental anomalies.
The genetic cause of atrophy is inherited from one or both parents as a result of genetic disorders: Leber atrophy, juvenile optic atrophy, optodiabetic syndrome, etc.
Vascular causes of the disease include hypertension, atherosclerosis, diabetes mellitus types 1 and 2, systemic lupus erythematosus, as well as several rare diseases: Behcet's disease, Horton's disease, Takayasu syndrome. Another reason for the triggering of atrophic changes in nerve fibers is large simultaneous blood loss [3][4][6].