Headache is a common problem faced by city residents. It occurs due to many reasons, including the environment, stress, malfunctions of the body, disturbed emotional balance, etc.
Regular yoga classes help you relax, restore your health, and make your thinking positive. Sets of exercises relieve muscle tension that negatively affects blood circulation in the brain. Yoga for illnesses helps to cope not only with the symptoms, but also relieves the causes of headaches.
Impact principle
Modern pharmacology offers a wide range of drugs that almost instantly eliminate pain and spasms. But this only masks the problem and prevents the organs from sending signals. Moreover, medications have side effects that lead to other problems.
A headache is a kind of signal that tells a person that the body is not working properly. Very often, spasms appear due to overstrain of the neck and back muscles. This is a common problem for modern people who spend most of the day sitting. Yogic exercises help relieve tension, normalize blood pressure and prevent headaches.
REFERENCE! Asanas and breathing practices eliminate the effects of stress, which also causes headaches. Yoga therapy focuses on gradual relaxation and slowing down. Complexes of various poses help improve the supply of oxygen to the brain and reduce the likelihood of migraines.
The effect of exercise on the development of a migraine attack
Migraine is one of the most common neurological diseases. In Europe alone, 15% of the population suffers from this disease. Migraine is a cyclical disorder characterized by recurrent attacks of headache, nausea, photophobia and phonophobia. Often headaches are aggravated by excessive physical activity. In most cases, attacks are accompanied by focal neurological symptoms. Migraine significantly affects the patient’s quality of life, affects performance and material costs (on average, about 1,200 euros are spent on combating migraine per year). In addition, it is also a risk factor in the development of cardiovascular diseases. A doctor has several treatment options for migraine, but in some cases they may be ineffective or have a significant list of side effects and contraindications. Lack of adherence to treatment is common among migraine patients. Thus, it can be said that there is a need for non-pharmacological treatments for migraine.
Regular exercise has many health benefits, and some studies have shown that these benefits extend to migraines. Regular exercise can reduce the intensity and frequency of migraine attacks. However, some people with migraines also report that exercise or sports are a trigger for the attack. This may be due to an increase in blood pressure during exercise. If exercise is a trigger, there are techniques to help you stay active and reduce your risk of developing a migraine attack.
Exercise can be used not only to combat migraines, but also to treat other chronic diseases. Interestingly, they can also influence conditions that are comorbid with migraine, such as depression, anxiety and insomnia.
On the other hand, physical activity may be the cause of the development of another attack. This is the reason for low physical activity among patients. In turn, physical activity is one of the diagnostic criteria for making a diagnosis according to the classification of the International Headache Society.
Relationship between exercise and migraine epidemiology
Previous studies have shown that low physical activity contributed to an increase in the incidence of headaches and exacerbation of migraines, and, conversely, sufficient physical activity contributed to a decrease in the incidence of headaches and exacerbation of migraines.
Led by Dr. Varkey, the Nord-Trøndelag Health Survey (HUNT) conducted one of the largest studies on this topic. This study (1984–1986) involved 22,397 people who did not suffer from frequent headache attacks and did not regularly use analgesics to treat them. This group of people was surveyed to determine physical activity and the nature of headaches. After 11 years, the same subjects were interviewed again. The study showed that in the group of subjects with active physical activity, the number of headache episodes was significantly reduced compared to the group with low physical activity.
Molarius et al [5] conducted a study among Swedish residents, including a random sample of 43,770 men and women aged 18 to 79 years, covering 58 municipalities throughout the country. The aim of the study was to evaluate the relationship of socioeconomic factors with the frequency of headache/migraine attacks. The study results showed that headache attacks were more common among physically inactive subjects.
Hagen et al. [6], in their study (over 12 weeks) concluded that VO2 Max (meaning the maximum volume of oxygen (in milliliters) per kilogram of body weight that a person can absorb in a minute at maximum physical activity) among patients with Migraines and tension headaches were significantly lower than in those studied who did not have frequent attacks of headaches.
Kinart et al. [7] evaluated 791 American Division I male and female basketball players and found a lower prevalence of migraine compared with the general population.
In the Korean study by Seok et al., a group of 136 patients with transformed migraine (TM) was followed for at least 1 year. The authors defined TM as a frequency of more than 15 migraine attacks per month over a 6-month period. The diagnosis of migraine was made according to with MOHD-II diagnostic criteria.
This study also included patients who abused drugs of NSAIDs more than 15 days per month for 3 months or a combination of analgesics, ergotamine, or triptan more than 10 days per month for 3 months.
The purpose of the study was to identify factors (eg, cessation of analgesic abuse, regular use of preventive medications, and lifestyle changes, including regular exercise and avoidance of caffeine, alcohol, and smoking) that play a pathogenetic role in the transition of TM to episodic migraine (defined by the authors as less than 8 headaches per month). A total of 95 patients (70%) developed TM into episodic migraine. The factor level that was significantly different between patients with episodic migraine and irregular migraine was p
Exercise as a trigger for another migraine attack: clinical evidence
The number of studies proving the involvement of physical exercise in the development of another migraine attack is not as large as it might seem at first glance.
Williams et al examined the prevalence of exercise-induced migraine among 129 New Zealand University staff and students aged 15 to 40 years. Eleven (9%) subjects experienced a headache meeting the International Classification of Headache Disorders-I (International Classification of Headache Disorders) criteria associated with migraine during or after vigorous physical activity.
A study was also conducted in one of the large US clinics. The subjects were 1207 patients aged from 13 to 80 years (average age 37.7 +/- 12 years). In 22%, physical activity was the cause of another migraine attack [8].
A little later, in a smaller, but no less informative, Dutch study of 103 patients with migraine, physical activity was the cause of the attack in a larger number of patients. In 38% of the subjects, migraine was in one way or another associated with physical exercise; in 17%, the attack began during exercise [9]. In addition, a study by Danish scientists who used provocative tests (in this case, active physical activity) showed that 4 out of 12 patients in whom exercise was the cause of migraine had another attack after exercise on a treadmill or stationary bicycle.
Among the study group of Swedish patients, 8 of 14 patients (57%) experienced migraine during vigorous aerobic exercise on a bicycle ergometer (first test). In 3 (21%) - during the second test with a treadmill. It is worth noting here that in 8 patients who suffered a migraine attack after bicycle ergometry, the predisposition to developing an attack was higher than in the remaining 6 people (p = 0.036).
Some studies have noted a high incidence of migraine co-occurrence with primary tension-type headache (hereinafter referred to as PHTN), which can appear after being outdoors in hot weather, at altitude within the last 48 hours, or after intense physical activity. And in principle, this is a common phenomenon among the population, and most often occurs among middle-aged people, approximately 0.2–12.3% [9]: Hanashiro et al. determined that the concomitance of migraine and PPH occurred in 158 of 2546 studied patients (6.2%). The high comorbidity of PPH and migraine can be observed in studies by other authors: Cheh et al. [24] among adolescents, such comorbidity reaches 30%, similar to the study by Ende-Kastelijn et al. [9], where this figure is 26% [11]. These authors concluded that despite the classification, PPH and exercise-induced migraine are very similar in symptoms, i.e. an attack of PHTH may be perceived as a migraine attack [9–11]
In a study characterizing the prevalence of headache in 1963 among Taiwanese adolescents, Chen et al. [11] determined that PHTH was more common in individuals with migraine compared with those without migraine [54.9% vs. 25.7%]. %, odds ratio (OR) 3.4, p
Exercise as a preventive treatment for migraine
Regular physical exercise plays an important role in the course of chronic diseases, since it can either prevent or even relieve various types of pain syndrome, for example, chronic neck and lower back pain, pain due to osteoarthritis, fibromyalgia and headaches [1].
The effectiveness of exercise as a preventative treatment for migraine has been examined in several studies. Some of the studies report a significant reduction in both pain intensity and a beneficial effect on the frequency and duration of migraine [14–18].
In a study of 480 medical students, Domingues et al. found a significantly lower rate of migraine-related disorders assessed by the MIDAS scale (p = 0.03) between those who exercised regularly (MIDAS: 15.49 ± 1.78) and those who did not exercise (MIDAS: 8.81 ± 1.40). Physical exercise included both aerobic and vigorous exercise. However, no difference in migraine prevalence was found between the two groups.
German scientists conducted a study on the effect of a 10-week aerobic training program on the nature of headaches and changes in cognitive functions of the brain [17]. As a result, a significant reduction in the number of migraine days per month (p = 0.01) and migraine attacks per month was determined (p = 0.001).In addition, cognitive functions of the brain, such as attention and speed of decision-making, also improved within 8 weeks of training.
Varkey et al. in Sweden developed an aerobic exercise program for untrained migraine patients and showed that it could safely
improve physical performance (increasing oxygen saturation in the blood) without aggravating the migraine. 26 patients followed a 12-week cycle ergometer program. The program was well tolerated by the subjects. Significant improvements were observed in attack frequency, pain intensity, patient quality of life, and drug absorption.
A randomized controlled trial was also conducted in 91 patients with migraine (migraine frequency 2–8 days/month), comparing the effect of aerobic exercise three times a week for 3 months with topiramate and rest. All three interventions were beneficial and equivalent to each other in reducing the frequency of migraine attacks, but side effects appeared only in the topiramate group.
Another comparative study in Brazil concluded that the combination of amitriptyline and aerobic exercise resulted in a reduction in the frequency, duration and intensity of headaches, depression and anxiety compared with amitriptyline alone among patients with chronic migraine [18]. Krøll et al. conducted a clinical trial in Denmark assessing the effects of a three-month aerobic exercise cycle using cycling and brisk walking among 26 patients with migraine and concomitant tension-type headache and neck pain [19].
Exercise resulted in a reduction in migraine headache activity, frequency, duration, and intensity, but not significantly relative to the control group. There is some evidence of the effectiveness of relatively anaerobic forms of exercise in the treatment of migraine.
In a study of 72 patients with migraine without aura, yoga therapy was randomly assigned. At the end of the study, a significant reduction in the frequency of migraine attacks was found (p
Pathophysiological theories/mechanisms of the influence of physical exercise on the development of a migraine attack
Hypocretin pathology
Hypocretin is produced by the hypothalamus and is involved in the regulation of sleep and wakefulness. Patients with migraine exhibit abnormalities in hypocretin metabolism, which affects the prodrome of migraine (the so-called aura) and manifests itself as excessive sleepiness, food cravings, yawning and fatigue [22]. Patients also often report that sleep can interrupt a migraine attack. [23]. Moreover, it was previously found that athletes often experience sleep disturbances [24]. Thus, active physical activity can influence the metabolism of hypocretin and contribute to the development of a migraine attack.
The harmful effects of lactate on energy metabolism
Anaerobic exercise causes a byproduct called lactate to accumulate in the body. Magnetic resonance spectroscopy has shown that the frequency of migraine attacks is directly related to increased lactate levels in the brain [25].
Calcitonin gene-related peptide (CGRP) is a neuropeptide circulating in the central and peripheral nervous system, the main function of which is vasodilation and transmission of pain impulses [26]. The concentration of this peptide increases during pain [27] and CGRP has been shown to be released during migraine attacks and return to normal levels after use of the antimigraine drug sumatriptan [28]. During exercise, CGRP levels increase and it is thought that this may be associated with muscle soreness [29]. However, CGRP is not measured during exercise in people with migraine, so its potential role as a mediator through which intense exercise may trigger migraine attacks needs further confirmation.
Migraine exacerbation during physical activity
During a migraine attack, there is increased activity of the sensory branches of the trigeminal nerve, which leads to the release of pro-inflammatory enzymes that can sensitize the tissues surrounding the arteries, particularly in the meninges.
Thus, pulsations that are not even felt under normal conditions can be felt as pain during a migraine attack. In this situation, every action that increases heart rate and/or arterial blood flow causes an increase in pulsations resulting in throbbing pain in patients. Therefore, most migraine patients, unlike patients with tension headaches, avoid normal physical activity during a migraine.
On the contrary, the absence of a temporal relationship between the ictal (attack-induced) pulsation and the arterial pulse indicates a minor role of the meningeal arterial pulsation in pain.
There is also confirmed evidence of the effect of increased intracranial pressure on the development of a migraine attack [30].
The therapeutic effect of exercise during a migraine attack
Endogenous opioids regulate pain sensitivity, i.e. during a migraine attack, their concentration increases at the end of the attack. Beta-endorphin is an endogenous opioid that is produced by the anterior pituitary gland and leads to analgesia by binding to pre- and postsynaptic opioid receptors (mainly mu receptors). After exercise, the level of beta-endorphin increases significantly only when a certain anaerobic threshold is exceeded [32–34], this threshold can be lower, but only if the exercise was performed for at least 50 minutes [35]. In the peripheral nervous system it appears to inhibit the release of substance P, which reduces the transmission of pain impulses, whereas in the central nervous system it acts on presynaptic membranes to inhibit the release of GABA. This leads to excess production of dopamine. It has been found that beta-endorphin levels are lower in migraine patients compared to healthy people. Its level is even lower in patients with chronic migraine [38]. However, research has shown that regular physical activity increases beta-endorphin levels [39]. Köseoglu et al. studied 40 women with migraine without aura who exercised for 6 weeks, 40–50 min 3 times per week at 60–80% of their maximum heart rate during headache periods. After measuring the amount of beta-endorphins in the subjects, the scientists concluded that after the workout, their levels doubled compared to the level before the workout. Performing regular exercise led to an increase in beta-endorphin, which likely contributed to the reduction in the number of migraine days from 2 to 1 per month.
One study looked at 40 women with migraine without aura. Some of them were assigned to the active group (i.e., 1 hour of moderate aerobic exercise three times a week) and some to the control group (where pharmacotherapy was used exclusively). In the active group, headache frequency decreased from 7.4 (standard deviation [SD] 2.9) to 3.6 (SD 1.6) days (p
It was observed that headache intensity in the active group decreased significantly compared to the control group (p 0.05) [15]. However, it was noted that regular aerobic exercise has a positive effect on sleep quality, psycho-emotional state, cardiovascular function and helps reduce excess weight.
These studies show that a person who regularly engages in aerobic exercise can alleviate the burden of migraines by reducing pro-inflammatory and increasing anti-inflammatory markers in the brain. Thus, people who stick to regular exercise despite some health challenges may become more influential in controlling migraines. However, the basic biological mechanisms of these processes are still unknown.
Conclusions and recommendations
Thus, the high prevalence of migraine, as well as the significant socioeconomic burden on patients and society as a whole, once again highlights the unmet need for therapeutic modalities for the treatment and prevention of migraine. An increase in comorbidities such as depression, anxiety and obesity have been associated with migraine. Thus, non-drug treatment is becoming even more popular in order to avoid polypharmacy or negative interactions of the drugs used. In addition, there are also patients whose migraine attacks do not respond to pharmacological treatment. Regular exercise has been suggested as a possible therapy for migraine. Their advantage is that they cost nothing in themselves, making them accessible to most migraine sufferers, as well as in low- and middle-income countries with low numbers of doctors.
Scientific research in this area, although somewhat limited, indicates positive results indicating that aerobic exercise has a positive therapeutic effect for migraine patients in both adolescents and adults, reducing the frequency and intensity of headaches, improving quality of life patients [16], has several significant benefits for general health (normalization of weight, sleep, psycho-emotional state, function of the cardiovascular system), including conditions that often accompany migraine (obesity, hypertension, sleep apnea, depression, anxiety), without causing side effects and does not require significant costs. Moreover, this method of treatment is suitable for people with low physical activity, which in itself causes an increase in the frequency of migraine attacks and the intensity of headaches.
Due to the lack of specific exercises for the treatment of migraines, a general principle of training can be outlined, which includes aerobic exercises: cycling and walking, eccentric or isometric exercises, it is also necessary to remember to warm up before training, which firstly reduces the risk of injury during training, and secondly, training on “cold muscles” can cause a migraine attack in people with this disease. The training program should be drawn up by a competent specialist, in order to avoid subsequent injuries, and with a frequency of 2-3 times a week. I would like to note that patients need to continue training despite the lack of effect at first.
Conclusion
Given the positive combination of effectiveness, minimal side effects, numerous benefits to overall health and significant financial savings, exercise programs can be considered an integral part of migraine therapy.
Literature:
- Daenen L, Varkey E, Kellmann M, Nijs J (2015) Exercise, not to exercise, or how to exercise in patients with chronic pain? Applying science to practice. Clin J Pain 31:108–114
- Irby MB, Bond DS, Lipton RB, Nicklas B, Houle TT, Penzien DB (2016) Aerobic exercise for reducing migraine burden: mechanisms, markers, and models of change processes. Headache 56:357–369
- Nadelson C (2006) Sport and exercise-induced migraines. Curr Sports Med Rep 5:29–33
- Lane JC (2000) Migraine in the athlete. Semin Neurol 20:195–200
- Molarius A, Tegelberg A, Ohrvik J (2008) Socio-economic factors, lifestyle, and headache disorders—a population-based study in Sweden. Headache 48:1426–1437
- Hagen K, Wisløff U, Ellingsen Ø, Stovner LJ, Linde M (2015) Headache and peak oxygen uptake: the HUNT3 study. Cephalalgia 36:437–444
- Kinart CM, Cuppett MM, Berg K (2002) Prevalence of migraines in NCAA division I male and female basketball players. National Collegiate Athletic Assoc Headache 42:620–629
- Kelman L (2007) The triggers or precipitants of the acute migraine attack. Cephalalgia 27:394–402
- Van Der Ende-Kastelijn K, Oerlemans W, Goedegebuure S (2012) An online survey of exercise-related headaches among cyclists. Headache 52:1566–1573
- Hanashiro S, Takazawa T, Kawase Y, Ikeda K (2015) Prevalence and clinical hallmarks of primary exercise headache in middle-aged Japanese on health check-up. Intern Med 54:2577–2581
- Chen SP, Fuh JL, Lu SR, Wang SJ (2009) Exertional headache—a survey of 1963 adolescents. Cephalalgia 29:401–407
- Darling M (1991) The use of exercise as a method of aborting migraine. Headache 31:616–618
- Lemstra M, Stewart B, Olszynski WP (2002) Effectiveness of multidisciplinary intervention in the treatment of migraine: a randomized clinical trial. Headache 42:845–854
- Osün Narin S, Pinar L, Erbas D, Oztürk V, Idiman F (2003) The effects of exercise and exercise-related changes in blood nitric oxide level on migraine headache. Clin Rehabil 17:624–630
- Dittrich SM, Günther V, Franz G, Burtscher M, Holzner B, Kopp M (2008) Aerobic exercise with relaxation: influence on pain and psychological well-being in female migraine patients. Clin J Sport Med 18:363–365
- Overath CH, Darabaneanu S, Evers MC, Gerber WD, Graf M, Keller A, Niederberger U, Schäl H, Siniatchkin M, Weisser B (2014) Does an aerobic endurance program have an influence on information processing in migraineurs? J Headache Pain 15:11
- Santiago MDS, Carvalho D de S, Gabbai AA, Pinto MMP, Moutran ARC, Villa TR (2014) Amitriptyline and aerobic exercise or amitriptyline alone in the treatment of chronic migraine: a randomized comparative study. Arq Neuropsiquiatr 72:851–855
- Krøll LS, Hammarlund CS, Linde M, Gard G, Jensen RH (2018) The effects of aerobic exercise for persons with migraine and co-existing tension-type headache and neck pain. A randomized, controlled, clinical trial. Cephalalgia.
- John PJ, Sharma N, Sharma CM, Kankane A (2007) Effectiveness of yoga therapy in the treatment of migraine without aura: a randomized controlled trial. Headache 47:654–661
- Elinoff V, Lynn SJ, Ochiai H, Hallquist M (2009) The efficacy of Kiko exercises on the prevention of migraine headaches: a pilot study. Am J Chin Med 37:459–470
- Rainero I, Rubino E, Gallone S, Fenoglio P, Picci LR, Giobbe L, Ostacoli L, Pinessi (2011) Evidence for an association between migraine and the hypocretin receptor 1 gene. J Headache Pain 12:193–199
- Bigal ME, Hargreaves RJ (2013) Why does sleep stop migraine? Curr Pain Headache Rep 17:369
- Hausswirth C, Louis J, Aubry A, Bonnet G, Duffield R, Le Meur Y (2014) Evidence of disturbed sleep and increased illness in overreached endurance athletes. Med Sci Sports Exerc 46:1036–1045
- Watanabe H, Kuwabara T, Ohkubo M, Tsuji S, Yuasa T (1996) Elevation of cerebral lactate detected by localized 1H-magnetic resonance spectroscopy in migraine during the interictal period. Neurology 47:1093–1095
- Arulmani U, MaassenVanDenBrink A, Villalón CM, Saxena PR (2004) Calcitonin gene-related peptide and its role in migraine pathophysiology. Eur J Pharmacol 500:315–330
- Onuoha GN, Alpar EK (1999) Calcitonin gene-related peptide and other neuropeptides in the plasma of patients with soft tissue injury. Life Sci 65:1351–1358
- Goadsby PJ, Edvinsson L (1993) The trigeminovascular system and migraine: studies characterizing cerebrovascular and neuropeptide changes seen in humans and cats. Ann Neurol 33:48–56
- Jonhagen S, Ackermann P, Saartok T, Renstrom PA (2006) Calcitonin gene related peptide and neuropeptide Y in skeletal muscle after eccentric exercise: a microdialysis study. Br J Sports Med 40:264–267
- Blau JN, Dexter SL (1981) The site of pain origin during migraine attacks. Cephalalgia 1:143–147
- Anselmi B, Baldi E, Casacci F, Salmon S (1980) Endogenous opioids in cerebrospinal fluid and blood in idiopathic headache sufferers. Headache 20:294–299
- McMurray RG, Forsythe WA, Mar MH, Hardy CJ (1987) Exercise intensity-related responses of beta-endorphin and catecholamines. Med Sci Sports Exerc 19:570–574
- Goldfarb AH, Hatfield BD, Armstrong D, Potts J (1990) Plasma betaendorphin concentration: response to intensity and duration of exercise. Med Sci Sports Exerc 22:241–244
- Langenfeld ME, Hart LS, Kao PC (1987) Plasma beta-endorphin responses to one-hour bicycling and running at 60% VO2max. Med Sci Sports Exerc 19:83–86
- Schwarz L, Kindermann W (1989) β-Endorphin, catecholamines, and cortisol during exhaustive endurance exercise. Int J Sports Med 10:324–328
- Guillemin R, Vargo T, Rossier J, Minick S, Ling N, Rivier C, Vale W, Bloom F (1977) Beta-endorphin and adrenocorticotropin are selected concomitantly by the pituitary gland. Science 197:1367–1369
- Sicuteri F (1978) Endorphins, opiate receptors and migraine headache. Headache 17:253–257
- Misra UK, Kalita J, Tripathi GM, Bhoi SK (2013) Is β endorphin related to migraine headache and its relief? Cephalalgia 33:316–322
- Schwarz L, Kindermann W (1990) Beta-endorphin, adrenocorticotropic hormone, cortisol and catecholamines during aerobic and anaerobic exercise. Eur J Appl Physiol Occup Physiol 61:165–171
- Dahl A, Russell D, Nyberg-Hansen R, Rootwelt K (1990) Cluster headache: Transcranial Doppler ultrasound and rCBF studies. Cephalalgia 10:87–94
- Olesen J (2008) The role of nitric oxide (NO) in migraine, tension-type headache and cluster headache. Pharmacol Ther 120:157–171
- Higashi Y, Sasaki S, Kurisu S, Yoshimizu A, Sasaki N, Matsuura H, Kajiyama G, Oshima T (1999) Regular aerobic exercise augments endothelium-dependent vascular relaxation in normotensive as well as hypertensive subjects: role of endothelium-derived nitric oxide . Circulation 100:1194–1202
- Varin R, Mulder P, Richard V, Tamion F, Devaux C, Henry JP, Lallemand F, Lerebours G, Thuillez C (1999) Exercise improves flow-mediated vasodilation of skeletal muscle arteries in rats with chronic heart failure. Role of nitric oxide, prostanoids, and oxidant stress. Circulation 99:2951–2957
Preventive asanas
The main yoga asanas, which allow you to avoid pain or significantly reduce the number of attacks, are aimed at relaxing and healing the areas of the body that provoke pain.
You should start the exercises by warming up your neck. Sit comfortably on a chair or on the floor with your legs crossed and your arms freely at your side. Raise your right hand above your head and reach your left ear. Slowly tilt your head to the right side. Apply light pressure with your hand and resist it with your head. After 60 seconds, straighten up and do the same on the other side.
IMPORTANT! First of all, attention is paid to the neck, spine, shoulder girdle and forearms.
Dog pose or dolphin pose helps release tension in your forearms and stretches your upper back. It is important to keep your breathing free and not strain your neck. Start on your knees, hip-width apart, with your hands on the floor and your wrists shoulder-width apart. Take a breath. Lower your elbows to the floor, slowly lift your hips and exhale. The heels should be parallel to each other. It is not necessary to place them on the floor if the stretch does not allow you to do so. Relax your neck, look at your feet and hold the pose for 3-5 breathing cycles.
Camel pose. Get on your knees, bend back, rest your palms on your feet. Do not push your hips forward; they should be perpendicular to the floor. Don't strain your neck, breathe freely. Hold the pose for 3-5 breathing cycles. This asana helps open the duct of the vertebral arteries and prevents headaches due to tension in the neck.
Exercise effectiveness
These three exercises must be performed regularly to avoid headaches. They are quite simple, accessible to a person with any level of training.
- The first exercise relaxes the forehead area, engages the legs and arms, and relieves tension from the neck muscles. To perform it, you will need a chair, the back of which must be placed against the wall and covered with a blanket. Stand facing a chair and press your palms against the wall, raising them just above your shoulders. Leave your feet hip-width apart. Step back until your arms are parallel to the floor. Rest your forehead against the back of the chair and lightly pull the top of your head toward the wall. If you are bothered by severe muscle tension in your legs, bend your knees slightly. Hold the pose for 1-2 minutes and slowly come out of it. Calm your breathing in Mountain Pose (Tadasana).
- The second exercise is similar to the inverted dog pose. Don't change your chair position. Place your palms on the seat and step back until your arms and torso are in line. Reach the top of your head towards the wall, stretching your neck. After 1-2 minutes, smoothly exit the pose and perform Tadasana again.
- To perform this asana, you must use a special block. It helps calm the mind. Get on all fours with your heels touching the wall. Place a block on the mat and assume the Downward-Facing Dog position. Place the upper part of the forehead on the brick. Breathe freely, do not strain your throat. After 1-2 minutes, relax in child's pose.
Reference! Yoga also helps eliminate and prevent the manifestation of unpleasant symptoms of hemorrhoids.
Camel Pose
This exercise relaxes the spine and shoulders well. If your headache is caused by tension in these areas, then it will certainly make you feel better.
Photo: istockphoto.com
Get on your knees, place them hip-width apart. Point the backs of your feet upward. Slowly arch your back without bending your hips - they should be at right angles to your shins. Place your palms on your heels and, pushing away from them, open your chest. In this case, the shoulders should be turned outward, and the shoulder blades turned inward. Stretch your neck and slowly lower your head. Stay in this position for 30 seconds, then raise your head, remove your hands from your heels and carefully straighten your back, returning to the starting position.
When performing the exercise, it is important to maintain calm breathing and try not to strain your stomach. If at the initial stage it is difficult for you to lower your hands to your heels, then place a cushion or a special block under your feet.
What to do if your head already hurts?
If you still have a headache or feel it approaching, try Viparita Karani asana. In this case, it should be performed not in its full form, but in a slightly modified form.
- lay a rug or blanket on the floor, sit sideways to the wall and bend your legs;
- lie on your back, bend your legs and place a sandbag on your feet, then straighten your legs, pressing them as much as possible against the wall;
- place the second bag of sand over your eyes and place your arms along your body;
- Relax completely and do not move for 15-20 minutes.
What yoga asanas are effective for migraines?
A calm yoga practice activates the parasympathetic nervous system, which is responsible for relaxation processes in the body. “I recommend doing relaxing yoga asanas—child’s pose, savasana, and anything that forces you to slow down and calm down,” says Sonya Matejko, founder of A Force of Nurture and a yoga teacher based in Los Angeles, USA . — It is also important to practice daily poses that gently stretch the muscles of the neck, shoulders and upper back. This improves blood circulation in the brain, which also helps combat migraines.”
Asanas can also be performed during an attack. But the most important thing for migraine prevention is to exercise regularly.
How to build a practice
- Start with light joint exercises.
- Perform the poses sequentially, staying in each pose for 2-3 minutes. If desired, you can hold the asanas longer.
- Finish the practice with savasana.
Child's Pose
Lower to your knees, then place your pelvis on your heels. Slide your palms forward, placing your forehead on the floor. In this position, relax the muscles of your neck, back and shoulder girdle. Close your eyes and observe your breathing for 2-4 minutes.
Forward lean
Stand up straight. As you exhale, bend forward and place your palms on the floor. Keeping your hands on the floor, straighten your knees. Relax your neck and shoulders, as if “hanging” with your body. Stay in this position for a minute. Return to the starting position, rest for another minute and repeat the asana.
Bridge Pose
Lie on your back, bend your knees, place your feet on the floor. Stretch your arms along the body, press the back of your head and shoulders onto the floor. Raise your pelvis and lower back so that your legs from your knees and your body form one straight line. Stay in this position for 2-3 minutes, then return to the starting position.
Breath work
Nadi Shodhana helps cleanse the energy channels of the body. To do this, sit with your back straight and relax. Use your thumb to close your right nostril and begin to inhale slowly through your left. After this, exhale even more slowly. Repeat the same with the other nostril. Do the practice for 1 minute.
Sheetali is a cooling breath that allows you to feel relief from headaches.
Sit cross-legged. Stick your tongue out of your mouth a little and roll it into a “tube”. Begin to slowly inhale through it and exhale through your nose, closing your mouth. Repeat 3-4 times without haste. REFERENCE! Pranayama or breathing exercises in yoga provide relaxation, relieve tension, improve blood circulation and calm the nervous system. They help get rid of headaches caused by stress or an immobile lifestyle.
Poses for Migraine Relief
Migraine is a neurological disease that is often accompanied by severe headaches. If you feel an attack coming on, perform Viparita Karani. But if you haven’t had time to do this, then try the practice of relaxation.
Legendary meditation course without payment We recommend! The most popular meditation course for beginners in Russian. More than 100 thousand people have already learned to meditate. Try it yourself. Read more.
Shavasana (dead man's pose) is suitable for this . It involves conscious relaxation of the body, relieves tension and restores strength. To complete this you will need 3 blankets and a bandage.
Fold the blanket into strips - one 30 cm wide, the other 70 cm long. Place one of them under the back area. Sit with your back to this stand with your knees bent. Wrap your head in a bandage or some kind of bandage.
Smoothly, supporting yourself with your hands, lie down. Your shoulders should only lightly touch the blanket under your head. Place your hands relaxed at a short distance from your body, palms up.
Raise your knees slightly and “throw” them onto the floor in a relaxed manner; do the same with your pelvis and chest. Close your eyes, take a deep breath in and out, and relax.
Feel each part of the body and relax it: start with the feet, move up the legs, then pay attention to the pelvis, back, abdomen, chest, hands and forearms.
It is very important to relax your neck, back of your head and face. Keep your breathing calm and observe the sensations in your body. ATTENTION! Audio accompaniment for performing guided Savasana.
After complete relaxation, try to let go of thoughts and remain in the pose for at least 5 minutes. When finished, bend your knees, turn over onto your right side, lie there for a while and slowly rise up.
Yoga therapy for migraines: advice from Sergei Agapkin
At the “Our Yoga” conference, which took place in early November at Prana, Sergey Agapkin shared his knowledge about methods of yoga therapy for migraines.
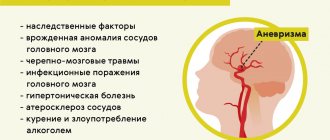
Features of migraines
About 15% of the total headache pattern is migraine. What makes migraines different from other types of headaches? Migraine is asymmetrical, occurring on one side. Tension headaches are dull headaches, while migraine headaches are sharp. Tension headaches are not characterized by any specific preceding period. Migraines are characterized by a period called aura, from the word “auros”, that is, breeze. People's sensitivity sharply worsens. Depending on the location of migraine foci in the brain, this may be an exacerbation of olfactory sensitivity, photophobia, intolerance to sounds, for some, skin sensitivity is exacerbated, even a light breeze can cause painful sensations in a person.
Migraine is 90% a hormone-dependent disease, so in 80% of cases migraine occurs in women. Migraine headaches are accompanied by pronounced vascular play.
Two phases of migraines
Migraine has two phases: in the first phase the blood vessels are dilated, and in the second they are narrowed. Research shows that when a person has a headache, the blood vessels dilate sharply and do not respond to the natural vasoconstrictor factors that the body produces. This is preceded by a period of vasoconstriction, that is, narrowing of blood vessels, when, on the contrary, there is no response to vasodilating factors. Anti-migraine drugs based on tryptomine cause a very persistent strong constriction of blood vessels. Sometimes people say that a certain drug does not help them, in fact they are taking it at the wrong phase. It is very important in what phase and in what form the drug is taken. The drug has a certain pharmacokinetics - the speed at which it is absorbed by the mucous membrane and enters the blood. By the time the drug gets into the blood, the phase can already change, and then the effect of the drug will most likely intensify the headache. This happens because the duration of the aura phase and the phase of the headache itself is unpredictable, the pharmacokinetics is predictable, but it is not always taken into account when the drug is prescribed.
There are 2 strategies for treating migraine headaches in neurology. One strategy, preventive treatment, is fraught with difficulties and is generally not particularly effective and is rarely used. The second is an abortive strategy, that is, interrupting an attack at the very beginning. The abortion strategy is based on two postulates. The first postulate is that at the first signs of the first phase, treatment must begin. The second postulate is that an uninterrupted attack automatically increases the duration and depth of the next one. Because each migraine attack is accompanied by an even greater stretching of the vascular wall, which gradually causes an increasingly stronger reaction each time. The most effective treatment is to interrupt the attack at the very beginning. At the initial stage, vasodilators are used, and if they do not have time, then when the pain begins, tryptamines are prescribed. Standard options like analgin do not work at all.
Yoga therapy for migraines
In yoga, there are a number of techniques that affect vascular tone, including the tone of cerebral vessels - techniques belonging to the class of pranayamas - hypocapnic techniques and hypercapnic techniques. Hypercapnia causes dilation of blood vessels, while hypocapnia causes leaching of carbon dioxide and constricts blood vessels. It must be taken into account that the longer a migraine lasts, the lower the sensitivity of blood vessels to carbon dioxide. The vessels become a little “frostbitten” and react with some delay. Two techniques are used - bhastra kumbhaka, that is, bhastrika, which is performed by hyperventilation, and kevala kumbhaka, which is performed with minimal ventilation of the lungs and leads to the accumulation of carbon dioxide. If they are started to be used at the appropriate phase, they can interrupt migraine attacks.
During the phase of dilation of blood vessels (when the migraine has already begun), we perform bhastrika in the classic version - intensively.
Yoga therapy in the aura phase
In the phase of vasoconstriction (pre-migraine phase), it is necessary to achieve the accumulation of carbon dioxide, so bhastrika is performed in a special way. There are 2 options: hypercapnia and expiratory retention, because carbon dioxide accumulates fastest when the retention occurs during exhalation. The second option is to reduce the volume of ventilation. This method is good because it does not cause any significant changes in blood circulation (when exhalation is delayed, venous return increases). When we hold with the glottis open in the neutral phase of breathing, no changes in hemodynamics occur. Sometimes a delay in exhalation gives a good effect, especially if the venous outflow is impaired, but this is not always necessary.
How to make Kevala Kumbhaka. There are 2 forces that oppose each other. The elastic force of deformation of the chest occurs during inhalation: when we inhale, the chest expands. We have relaxed the muscles that are responsible for inhalation, and involuntary exhalation occurs. After which the involuntary exhalation has ended and we can continue if we tense the abdominal muscles, internal intercostal muscles and deform the chest in the other direction - squeeze it. If we exhale, we inhale involuntarily; when this occurs, our pressure equalizes again. The position between inhalation and exhalation - the neutral position - is the most comfortable for us. The glottis is open, there is no need to block it. At a certain depth of inhalation, we do not ventilate the lungs at all. The most important thing is to find a comfortable delay value and a comfortable breathing depth. Inhale, exhale briefly with your mouth open. Let's take a deep breath. We start the delay from 3 seconds, adding 1 second at each cycle (we reach 20 seconds). We do not exhale. We gradually reduce the depth of inspiration.
At a certain moment, you will feel the first symptoms of hypocapnia - redness of the skin begins, a vascular reaction such as mild skin itching occurs, it becomes hot, and vasodilation occurs. If you continue at the same pace for about 10 minutes, a state of inhibition will arise, that is, you will begin to fall asleep. After about 10 minutes, carbon dioxide begins to affect the brain like a tranquilizer. The first 5 minutes are usually a phase of excitation, a gradual increase in CO2 levels leads to activation of the sympathetic-adrenal system, but we try to get around this by changing the depth of breathing and reducing the duration of the delay, and gradually from 5-7 minutes CO2 accumulates and the exact opposite reaction occurs, that is, braking. The brain begins to shut down, as when taking phenazepam, and it becomes very warm. If the duration of the aura is more than 10 minutes and you fall within this duration, then you will receive a complete disappearance of further symptoms. If the aura phase is shorter or you somehow did not get into it or started to perform too hard and you became excited, then, on the contrary, the attack may begin faster than it should.
Yoga therapy in the pain phase
If we do not get into the aura phase, another strategy is used - hyperventilation techniques. Specific movements, as when performing bhastrika, are not necessary. In our case, we use deep breathing in a fast rhythm. Usually a person breathes shallowly - diaphragmatic breathing, using far from the entire volume of his lungs (about 15%). If you do the same amount of movement per minute, but use your full lung capacity, you will reach a state of hyperventilation. It is impossible to confuse the symptoms: dizziness begins, sometimes coldness occurs in the extremities, in some cases sound, auditory and other hallucinations may appear, but this is if you get carried away too much. In our case, 10 approaches of 10 inhalations and exhalations each are sufficient. You can breathe through your mouth because your nose slows down your breathing.
How to determine the cause of a headache? This should be done by a neurologist. Not the first one that came along, of course, but a good one. There is an international classification of headaches and based on certain signs the cause is easy to determine. Moreover, it is possible to determine the causes even outside the exacerbation phase.
On Wikipedia there is a classification of headaches and a person himself can determine the type of pain based on the characteristic symptoms. Without being a neurologist, it is not at all difficult to determine the type of headache.
Recorded by: Masha Pisarevich