Clinical forms and classification of meningococcal infection
Meningococcal infection is characterized by large polymorphism, which is associated with the pathogenesis of the disease.
- Clinical forms of the disease are divided into localized and generalized. Localized forms include meningitis and nasopharyngitis, generalized forms include meningococcemia with rashes (typical form) and without rashes (atypical form).
- Localized and generalized forms can occur without metastasis to internal organs and with metastasis (meningitis, meningoencephalitis - the most common forms and pericarditis, myocarditis, arthritis, pneumonia, iridocyclitis and other rare forms).
- According to the severity of the course, meningococcal infection is divided into mild, moderate, severe and very severe. The degree of toxicosis, adrenal insufficiency, the rate of progression and severity of signs of damage to the central nervous system, the development of disseminated intravascular coagulation syndrome and infectious-toxic shock are the main criteria for the severity of meningococcal infection.
- If the duration of the disease is up to 3 months, they speak of an acute course, more than 3 months - a protracted course, and more than 6 months - a chronic course. The chronic form of menigococcemia and meningitis can have a relapsing course.
Rice. 2. The photo shows meningococcal infection in children. One of the main symptoms of the disease is a rash. Minor hemorrhages in the skin with meningococcal infection (left) and extensive bruises in a child with severe meningococcal sepsis (right).
Signs and symptoms of meningococcal infection in heart disease
Meningococcal toxin contains an allergenic substance, which leads to pronounced sensitization of the body from the moment it colonizes the nasopharynx. The formed immune complexes settle on the walls of blood vessels, increasing the damaging effect (Schwartzman-Sanarelli syndrome). Sensitization of the body underlies the development of arthritis, nephritis, pericarditis, episcleritis and vasculitis.
Meningococcal carditis accounts for half of all cases of damage to internal organs due to meningococcal infection. Toxic damage to the heart affects the endocardium, pericardium and myocardium. The contractility of the heart muscle decreases, and the heart rate increases. Hemorrhages into the heart muscle, tricuspid valve and subendocardial space lead to the development of cardiac weakness, which is often the cause of death of the patient.
When infection enters the pericardium, purulent pericarditis develops. On auscultation, a pericardial friction rub is heard.
Elderly people often develop myocardiosclerosis after an illness.
Rice. 13. The photo shows hemorrhages in the endocardium (left) and pericardium (right) with meningococcal sepsis.
Meningitis
The source of the disease are patients with generalized forms of meningococcal infection, acute nasopharyngitis and “healthy” carriers.
There is a fairly wide ratio between patients and bacteria carriers (1:2000 - 1:50,000). During periods of outbreaks, up to 3% of the population of bacteria carriers is registered, during epidemics - up to 30%. The carrier period is about 3 weeks. In 70%, bacterial carriage ceases within 1 week.
In patients with chronic diseases of the nasopharynx, this period is significantly longer. The most virulent strains are isolated by patients with generalized forms. Despite this, their rapid hospitalization and isolation do not have such an impact on the spread of infection as it does in “healthy” carriers.
Meningitis carriers are identified during mass examination of individuals from foci of the disease or accidentally, during examination of smears taken from the mucous membrane of the nasopharynx. Carriers of meningococci do not have any symptoms of the disease. The more severe the epidemic situation, the more carriers of the infection are identified in groups.
Out of 200 bacteria carriers, 1 bacteria carrier gets sick.
Rice. 3. The mechanism of transmission of meningococcal infection is aerosol (droplet).
Features of the rash
When a toxic substance is produced, the pathogen becomes a poison for the vascular system. A hemorrhagic rash is formed when toxins influence blood vessels, as a result of which their walls become maximally permeable.
Why can our articles be trusted?
We make health information clear, accessible and relevant.
- All articles are checked by practicing doctors.
- We take scientific literature and the latest research as a basis.
- We publish detailed articles that answer all questions.
Often spots appear in generalized forms of meningococcal infection, often immediately after infection.
Spots appear on the following areas of the body:
- shin;
- buttock area;
- feet;
- Hands;
- shoulders;
- forearms.
Externally, they may have an unnatural star-shaped shape. The size of the spots may vary.
- Small petechiae are small pinpoint hemorrhages.
- Large ecchymoses are bruises that can reach 6 centimeters or more in diameter.
Formations of a dense structure protrude slightly above the surface of the skin.
Based on the nature of meningitis, the doctor can determine the severity of the pathology. Sometimes the doctor can visually predict the type of pathogen based on the rash.
With severe development, spots are located throughout the body. On the extremities, rashes appear in the form of minor hemorrhages, which have uneven but clear contours. Outwardly, they initially look like cadaveric spots, and then the color of the rash can change from dark red to bluish.
- Is meningitis visible on CT scan?
Very severe cases of the disease are characterized by extensive hemorrhages of the vessels of the extremities, dark spots. They are formed from the feet to the knees, from the hands to the elbows. With such signs, the patient most often dies.
In most cases, the face does not develop a rash. In this case, hemorrhages can affect:
- ears;
- cheeks;
- tip of the nose.
The skin between the rash spots has a pale tint.
At the initial stage of development of the disease, a hemorrhagic rash may appear in the form of spots and nodules, which go away after 2-3 days.
It can often be observed that along with a skin rash, hemorrhages form on the oral mucosa, sclera, and conjunctiva.
Not all spots due to the disease appear simultaneously. The disease is characterized by the formation of new components of the rash, where areas of the skin are already affected, and hemorrhages increase.
Over time, small hemorrhagic formations become pigmented and then disappear. If these are large rashes, then as the disease develops they die, becoming covered with crusts over time. Once peeled off, these crusts leave scars on the skin that can vary in depth.
Signs and symptoms of meningococcal nasopharyngitis
Meningococcal nasopharyngitis can be an independent disease or indicate the prodromal period of purulent meningitis. It accounts for up to 80% of all forms of meningococcal infection.
The infectious process in meningococcal nasopharyngitis begins from the moment bacteria colonize the mucous membranes of the nose and pharynx. Activation of local protective mechanisms leads to the cleansing of mucous membranes from bacteria. The level of immunoglobulins (protective antibodies) increases in the blood, which are able to cleanse the body of microbes that have entered the bloodstream in small quantities. When the disease occurs, bacteria overcome local defenses and penetrate the submucosal layer. The disease develops. The incubation period for meningococcal infection averages from 4 to 6 days (2 - 10 days).
- A mild course of meningococcal nasopharyngitis is characterized by a slight increase in temperature or its absence, moderate headache, pain when swallowing, and sometimes hoarseness. A constant symptom of the disease is nasal congestion and mucopurulent discharge. The posterior wall of the pharynx is hyperemic, often with a bluish tint, edematous, and hyperplasia of lymphoid follicles is noted. Often patients who have a mild course of the disease do not seek medical help.
- As the symptoms of intoxication increase, body temperature rises to 38 °C. The appearance of at least single hemorrhagic rashes on the transitional fold of the conjunctiva of the lower eyelid and the skin indicates the generalization of the infectious process.
- Diagnosis of meningococcal nasopharyngitis based only on the clinical picture is difficult.
Rice. 4. The photo shows meningococcal nasopharyngitis.
Causes and symptoms
The initial sign of the development of a dangerous disease is a rash.
It can appear in the following places:
- sides;
- hips;
- shin;
- Feet;
- knees;
- forearms and hands;
- in rare cases on the face.
The rash appears due to pathogenic bacteria and viruses They cause an inflammatory process in the meninges, and this, in turn, affects the blood vessels. In particular, the capillary membranes are affected.
All this leads to the formation of local hemorrhage. This type of rash is commonly called hemorrhagic. In most cases, it makes itself felt with bacterial meningitis.
Reference! With the viral type of meningitis, immediate damage to the vascular endothelium occurs, which leads to a rash on the baby’s body.
By the way, not all parents pay attention to this symptom. Patients are admitted to the hospital already at the stage when a severe headache makes itself felt, body temperature rises, and frequent vomiting is present.
With meningitis, the rash is called erythema due to its characteristic appearance. Their appearance is explained by the fact that meningococcal toxin blocks blood vessels and increases the permeability of their walls.
Meningococcal meningitis
Meningococcal meningitis most often occurs in children aged six months to 10 years. It accounts for 10 to 12% of all generalized forms of meningococcal infection. In this case, a rash with meningitis will be an unfavorable prognostic sign. The incubation period for meningococcal meningitis is usually 4 days, but in some cases it can range from 2 to 10 days.
How does meningococcal meningitis develop?
Damage to the central nervous system is based on vascular damage by meningococcal toxins with the subsequent development of cerebral edema, and the penetration of bacteria through the blood-brain barrier, ethmoid bone and nerve sheaths leads to the development of purulent inflammation. The meninges swell, the convolutions smooth out, pinpoint hemorrhages and stasis develop, and blood clots form. The pathological process can spread to the cranial nerves. When the region of the bottom of the fourth ventricle of the brain is involved in the process of stem formations, breathing and cardiac activity are disrupted.
Rice. 5. The photo shows a view of the brain with meningococcal meningitis.
Rashes as a sign of other diseases
Doctors remind that it is not only meningitis that causes a rash to appear on the skin. You need to know how to distinguish rashes from other ailments:
- chickenpox. With this disease, the rash is more blistering and covers almost the entire body of the child. In addition, he complains of constant itching.
- measles. In this case, the rash appears on the face; with meningitis, this localization is quite rare.
- various allergic reactions. The spots have a redder tint, and the patient does not have a general infectious syndrome.
- rubella. With rubella, the spots do not merge, and the rash does not appear at the beginning of the disease, but as it progresses. In addition, with this disease a person develops a runny nose and sore throat;
- scarlet fever. This disease is provoked by streptococci, they also act as the instigators of meningitis. However, this disease does not cause itching.
- pyodemia. Here formations can spread throughout the body. It looks like bubbles.
Important! If any redness appears, regardless of the disease, you should consult a doctor.
The rash with meningitis is pronounced, but not everyone can recognize it at an early stage. Mostly, patients go to the doctor when other symptoms become apparent. The localization and nature of the rash helps to diagnose a dangerous disease in time. It must be treated exclusively in a hospital setting.
Signs and symptoms of meningococcal meningitis in children and adults
The first signs of meningococcal meningitis
Meningitis in 25% of cases has an acute onset. In 45% of cases, the disease begins with nasopharyngitis. Body temperature rises to 39 - 40°C. Then pain appears in the frontal, temporal, and less often occipital regions. The headache quickly becomes painful, pressing, bursting in nature. Appetite decreases and then disappears. Nausea and vomiting appear, which does not bring relief.
Signs and symptoms of meningococcal meningitis during the height of the disease
The disease begins with damage to the soft and arachnoid membranes of the brain. After 12 hours, symptoms of meningeal irritation appear, abdominal, periosteal and tendon reflexes decrease, and their unevenness is noted. Meningitis syndrome develops. The patient takes a special position: lying on his side, bends his legs and throws back his head. General weakness gradually increases, pain appears in the eyeballs, aggravated by movement.
Increased sensitivity (hyperesthesia) develops to all external stimuli - photophobia, painful sound perception. Lethargy and lethargy develop, sleep is disturbed. In severe cases, a state of stupor, stupor and coma develops. In the first days of the disease, symptoms of damage to the cranial nerves appear - facial, oculomotor, trigeminal and hypoglossal.
Rice. 6. If the membranes of the brain are damaged, the patient takes a special position: lying on his side, bends his legs and throws back his head.
Signs and symptoms of meningococcal infection in joints
Joint damage due to meningococcal infection is recorded in 5 - 8% of cases. More often one joint is affected, less often two or more. The wrist, elbow and hip joints are usually affected. Initially there is pain and swelling. With delayed treatment, the inflammation becomes purulent, which leads to the development of contractures and ankylosis.
Rice. 14. Arthritis due to meningococcal infection.
Signs and symptoms of meningoencephalitis
Meningoencephalitis is a rare form of meningococcal infection. It accounts for 3 to 6% of all cases. The disease is always severe. General intoxication syndrome is combined with meningeal and encephalic syndromes. In recent years, a combination of meningoencephalitis and meningococcemia—acute meningococcal sepsis—has been observed.
- Serous inflammation of the meninges quickly acquires the character of purulent inflammation. The inflammatory process spreads to the white matter of the brain. After 5 - 8 days, the pus turns into a fibrous mass.
- After 12 hours, symptoms of meningeal irritation appear, abdominal, periosteal and tendon reflexes decrease, and their unevenness is noted.
- General cerebral symptoms increase rapidly. Psychomotor agitation, auditory and visual hallucinations and delirium are replaced within a day by a deep disturbance of consciousness (stupor).
- As the symptoms of intoxication and cerebral edema decrease, signs of encephalitis appear. Focal cerebral insufficiency manifests itself in the form of damage to the cranial nerves - facial, oculomotor, trigeminal, sublingual and auditory; cortical and subcortical paresis and paralysis develop. Sometimes convulsions appear, which are general or local in nature, the psyche is disturbed, amnesia develops, auditory and visual hallucinations, depression or euphoria appear.
- There are moderate signs of changes in the functioning of the cardiovascular system. When the vasomotor center is involved in the pathological process, bradycardia occurs, and sometimes cardiac arrest is recorded.
- With hyperthermia, increased breathing is observed. During convulsions, short-term cessation of breathing may occur. Damage to the respiratory center leads to respiratory arrest.
The disease lasts from 4 to 6 weeks. In case of timely and adequate treatment, the prognosis is favorable. With late diagnosis and untimely treatment, the prognosis of the disease is unfavorable. Fatalities are common. Surviving children have epilepsy, delayed psycho-motor development and hydrocephalus. One of the severe complications of meningoencephalitis is inflammation of the ependyma of the ventricles of the brain. Damage to the auditory nerve can result in deafness.
In children suffering from rickets, malnutrition, and exudative diathesis, a protracted course (up to 2 months) of the disease is noted. There are also cases of long-term meningoencephalitis. The reasons for the chronicity of the pathological process have not been sufficiently studied.
Rice. 7. The photo shows purulent meningitis.
Signs and symptoms of meningococcal infection in the lungs
When the vessels of the lung tissue are damaged, a specific inflammation develops - meningococcal pneumonia. The disease develops against the background of severe intoxication.
The liquid sweats into the lumen of the alveoli, innervation is disrupted, the level of affinity of hemoglobin for oxygen decreases, respiratory failure and pulmonary edema develop, and the pleura may be affected. Initially, there is a focal lesion, but over time the infection spreads to the entire lobe of the lung. When you cough, a large amount of sputum is produced.
Recovery from meningococcal pneumonia is slow. The patient has been bothered by a cough for a long time, and asthenia develops.
Complications of meningococcal meningitis and encephalitis
During the acute period of the disease, such serious complications as intracranial hypertension, cerebral edema, infectious-toxic shock, subdural effusion, cerebral infarction, sensorineural hearing loss and diencephalic dysfunction are recorded. Infectious-toxic shock, ependymatitis, edema and swelling of the brain can cause death.
Acute edema and swelling of the brain
Acute edema and swelling of the brain occur at the end of the first day of the disease or the beginning of the second, more often with purulent meningitis, less often with meningococcal sepsis and are the main causes of death of the patient.
The development of this complication is based on toxic damage to the blood vessels of the brain with subsequent disruption of hemodynamics and metabolic processes. The first signs of acute edema and swelling of the brain are severe headaches, convulsions, psychomotor agitation, repeated vomiting and loss of consciousness.
Wedging of the brain into the greater occipital space leads to its pinching. At the same time, the pulse quickens, arrhythmia occurs, blood pressure becomes labile, breathing is noisy, the face becomes hyperemic, cyanosis develops, and the patient is bothered by severe sweating. Impaired breathing leads to hypoxia, hypocapnia and respiratory alkalosis. Pulmonary edema followed by respiratory arrest is the cause of death.
Dehydration therapy and parenteral administration of large doses of the potassium salt of benzylpenicillic acid in young children can lead to the development of cerebral hypotension. Intracranial pressure drops sharply, the amount of fluid in the ventricles of the brain decreases, the large fontanelle sinks in infants, facial features become sharpened, eyeballs sink, convulsions appear, blood pressure drops, and tendon reflexes fade. When the spinal canal is punctured, cerebrospinal fluid leaks out in drops, and cerebral collapse develops. Paralysis of the respiratory center leads to respiratory arrest.
Rice. 8. Meningitis in a child, complicated by acute edema and swelling of the brain.
Ependymatitis
When the inflammatory process spreads to the membrane lining the inside of the ventricles of the brain, ependymatitis develops. Complications can develop at different stages of the course of meningitis.
The clinical picture of ependymatitis is similar to that of meningoencephalitis. Drowsiness, prostration, stupor or coma, increasing hypertonicity, convulsions, trembling of the limbs, hyperesthesia and persistent vomiting are the main symptoms of this complication. In small children, a large fontanel bulges and the stitches may come apart. The cerebrospinal fluid turns yellow and contains a large amount of protein, meningococci and polynuclear cells.
Prolonged course of the disease and unsuccessful therapy for ependymatitis leads to the development of hydrocephalus and pyocephaly.
Increased intracranial pressure can lead to displacement of the brain with subsequent compression of the medulla oblongata. Death occurs from respiratory paralysis.
Rice. 9. The photo shows hydrocephalus in a child that developed as a result of meningococcal meningitis.
Treatment
If rash manifestations lead to the development of a hyperthermic state, severe pain, then urgent hospitalization and medical attention are required. If no adequate action is taken in the near future, the consequences can be very dire.
When treating meningeal infection, antibiotic therapy is prescribed. Using antibiotics, it is possible to stop the pathogenic microflora that led to the development of the disease. After hospitalization, the patient is placed in the inpatient department of the hospital. Further treatment is as follows :
- The doctor prescribes bed rest with a gentle diet for the patient.
- Antibacterial drugs. Prescribed drugs with low, medium and increased permeability. The most effective include: Amoxicillin, Cefuroxime, Ketoconazole, Clindamycin. The dosage is determined individually. But the duration of therapy should not be longer than 7-10 days, as addiction occurs.
- In addition to antibacterial therapy, antiviral drugs are prescribed.
- The combination of desensitizing therapy with anti-inflammatory therapy will alleviate the patient’s condition and relieve unpleasant symptoms.
The therapeutic course for any age category will be at least 10 days. If there are complicated forms, the duration of treatment may increase. As soon as the patient is discharged from the hospital, he should prepare for long-term home treatment. For some patients with meningococcal pathology, recovery requires 1 year. Read more about emergency care and nursing care for meningitis in this article.
There is a vaccine against meningitis . It can prevent the development of this dangerous disease. Vaccination is required in places where there is a regular outbreak of the disease.
- Rehabilitation after meningitis: recovery of the body and possible complications
TIP : When a skin rash is accompanied by a high fever and severe headache, you need to go to the hospital as soon as possible. This condition means that life is counted by the clock.
Consequences of meningitis and encephalitis
The prognosis for meningococcal meningitis in the case of timely and adequate treatment is favorable. In case of delayed diagnosis and delayed treatment, serious complications develop.
The consequences of meningitis are unpredictable and varied. Currently, complications of the disease associated with organic brain damage - hydrocephalus, mental retardation, dementia and amaurosis (damage to the optic nerve and retina of the eye) are very rarely observed. Complications of a functional nature are more often observed - asthenic syndrome and mental retardation. Complications of a functional nature are more often observed: asthenic syndrome, neurosis-like states, mental retardation.
Rice. 10. The photo shows the consequences of meningitis - damage to the VI pair of cranial nerves (convergent strabismus).
Cerebrasthenic syndrome
Emotional-volitional and behavioral disorders, headaches, sleep disorders, autonomic disorders and headaches are the main components of cerebrasthenic syndrome.
Cerebrasthenic syndrome, as a consequence of meningitis, manifests itself in two forms - hyperdynamic and hypodynamic.
The hyperdynamic form of cerebrasthenic syndrome is characterized by increased excitability, motor disinhibition, uncontrollability, and emotional lability. Often children begin to show aggression and cruelty that is unusual for them, they fight and offend animals.
The hypodynamic form of cerebrasthenic syndrome is characterized by lethargy, fearfulness, skittishness, timidity and indecisiveness, lack of initiative, and increased emotional sensitivity.
Behavioral disorders lead to exhaustion and fatigue over time. With complete preservation of intelligence, children begin to study poorly.
Neurosis-like conditions
Neurosis-like conditions, as consequences of meningitis, are characterized by monotony of manifestations and rigidity of the course.
Young children develop vegetative visceral syndrome, manifested by regurgitation, unstable stools, marbling of the skin, etc. Their sleep is disturbed, it becomes superficial and restless.
Children aged 4 to 7 years old develop obsessive movements, stuttering, night terrors, and enuresis.
Older children develop neurasthenia, sometimes hysteria and obsessive-compulsive neurosis, and vegetative-vascular dystonia.
Headaches are constant. They are provoked by overwork and anxiety. The pain is moderate in intensity, combined with dizziness, pale skin and sweating.
Hypothalamic dysfunction syndrome
Autonomic disorders, as a consequence of meningitis, are sympathetic, parasympathetic and mixed.
Rapid pulse, increased blood pressure, dry and pale skin, chilly legs, dry mouth, periodic increases in body temperature and white dermographism are the main manifestations of sympathicotonia.
Slow pulse, decreased blood pressure, increased salivation, increased intestinal motility, red dermographism are the main manifestations of parasympathicotonia.
Often the same child experiences symptoms of both types of autonomic disorders. The development of neuroendocrine metabolic syndrome is characterized by the development of obesity, edema and delayed puberty. If thermoregulation is disturbed, prolonged low-grade fever, sometimes hypothermia and chill-like hyperkinesis are recorded. With neurotrophic syndrome, baldness or excess hair growth appears in areas of the skin that are not typical for these areas (hypertrichosis), dry skin, and brittle nails. With neuromuscular syndrome, general and muscle weakness and adynamia appear.
Intracranial hypertension syndrome
Hypertension syndrome, as a consequence of meningitis, is manifested by headaches, dizziness and often accompanied by vomiting. Headaches appear in the morning and are paroxysmal in nature. Intracranial hypertension syndrome develops 2 to 6 months after the onset of the disease.
Focal disorders of the central nervous system
Focal disorders of the central nervous system are manifested by central paresis, damage to individual cranial nerves and cerebellar disorders, which respond well to treatment.
3 to 6 months after treatment, epileptiform seizures of various types may develop.
Rice. 11. The photo shows epileptiform seizures in children.
Cerebrasthenic syndrome
Cerebrasthenic syndrome, as a consequence of meningitis, is manifested by general weakness, increased fatigue, weakening of general reactions, decreased memory and dissipation of attention.
Rice. 12. Meningitis often occurs against the background of meningococcemia (meningococcal sepsis).
Laboratory diagnosis of meningococcal meningitis
- In the blood there is a significant increase in the number of leukocytes and neutrophilic granulocytes, and the erythrocyte sedimentation rate.
- During a spinal puncture, the cerebrospinal fluid is cloudy, flows out under pressure, and often has a greenish tint. With purulent meningitis, there is a significant increase in cellular elements in the cerebrospinal fluid (pleocytosis), a decrease in the content of sugar and chlorides.
- A smear prepared from the cerebrospinal fluid of a patient with meningitis reveals meningococci.
Rice. 13. The photo on the left shows the appearance of cerebrospinal fluid during meningitis. In the photo on the right, meningococci are obtained from the cerebrospinal fluid (bacterioscopy) of a patient with meningitis.
- Additional research methods include electroencephalogram (EEG), brain computed tomography (CT), neurosonography (NSG), color Doppler mapping, etc.
- If necessary, doctors of different specialties are involved in examining patients - ophthalmologists, otolaryngologists, neurologists.
Rice. 14. An electroencephalogram allows you to detect structural changes in the brain.
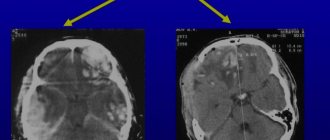
Rice. 15. Computed tomography of the brain allows one to detect the presence of hematomas, hydrocephalus and other space-occupying lesions localized in the brain.
What does it look like?
Almost immediately, a characteristic rash can be noticed on the child’s skin.
What does she look like?
At the very beginning, the rash has a red tint, but then turns blue.
In children, rashes appear first on the feet, and then begin to spread throughout the entire skin.
In this case, the child should be hospitalized and antibacterial therapy should be started.
Sometimes individual elements turn into quite large spots.
Meningitis spots are a sign of sepsis . If immediate antibiotic therapy is not started, death can occur.
The rash often becomes pigmented and then disappears. Sometimes crusts form, which are subsequently rejected on their own. In their place, shallow skin defects will remain for some time.
Photo
Read more about the meningitis rash in the photo:
Red rash on back