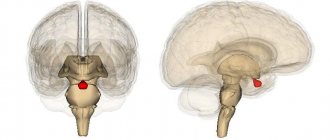
Frontal lobe syndrome (also frontal (neuropsychological) syndrome; personality disorder of organic etiology (according to ICD-10)) is a natural combination of symptoms caused by massive (mainly bilateral) damage to the frontal lobes of the brain. In accordance with the teachings of Luria A.R. about three functional blocks of the brain, the frontal lobes are components of the third functional block of the brain - the block of “programming”, regulation and control of activity. Thus, in general terms, frontal syndrome can be defined as a syndrome of dysfunction of programming, regulation and control of mental activity.
According to ICD-10, it refers to personality disorders of organic origin.
General characteristics of the syndrome of lesions of the frontal lobes of the brain
In patients with pronounced frontal syndrome, the performance of specific operations, the ability to perform mental actions, storage and use of the available stock of knowledge remain intact, however, it becomes impossible to use them in an appropriate way in accordance with a consciously set goal. These symptoms are most pronounced in the case of massive (bilateral) damage to the frontal lobes. When the frontal lobes are damaged, patients are not able to independently carry out any program of action, and are also not able to act in accordance with a ready-made program given to them in the instructions; the regulatory function of speech is impaired. These disorders occur against the background of personality changes: in a patient with damage to the frontal lobes of the brain, the formation of motives mediated by the speech system and intentions to perform certain forms of conscious activity are disrupted, which spreads and affects the entire behavior of the patient. The conscious, purposeful behavior of patients with lesions of the frontal lobes is disintegrated and replaced by less complex forms of behavior or inert stereotypes. Conditions that contribute to the loss of behavior programs are strong external stimuli; volitional behavior in such patients is replaced by field behavior (pathological, uncontrolled susceptibility to external influences), voluntary actions by involuntary ones.
Materials and methods
Participants
The study recruited 30 patients from Zhu Jiang Hospital of Southern Medical University who met the following criteria:
- age from 60 to 70 years;
- using the right hand as the leading hand;
- the presence of neurological symptoms and corresponding brain damage;
- being in the recovery period (from 3 months to 1 year) after a stroke with stable symptoms;
- a single infarct zone measuring from 3 to 5 cm, localized in the right frontal lobe;
- patients are lucid and able to interact with the interviewer;
- NIHSS score no more than 6 points;
- Barter index score more than 60 points;
- no history of previous ischemic or hemorrhagic strokes;
- no psychiatric history, no episodes of drug abuse.
Each patient underwent a clinical interview with an experienced neuropsychologist, who diagnosed depression in accordance with DSM-IV criteria. Depression severity was assessed using the HAMD-24 scale. As a result, patients were divided into two groups:
- patients with post-stroke depression (13 people): meeting the criteria for depression according to DSM-IV and a score on the HAMD-24 scale of more than 17 points;
- patients without post-stroke depression (17 people).
All patients participating in the trial also underwent assessment of cognitive function (MMSE) and vital activity (Barthel index).
Neuroimaging
Each patient underwent MRI and resting fMRI, each examination lasting 6 minutes.
Voxel-based morphometry
Voxel-based morphometry is a neuroimaging method that can reflect the volumetric density of the cerebral cortex and uses specialized software for this (in this case, SPM8). Voxel-based morphometry involves post-processing of MRI data.
Morphometry is performed in several stages:
1. Checking neuroimaging data for the presence of artifacts, structural abnormalities and pathologies, and identifying the main structures of the brain: gray and white matter, cerebrospinal fluid;
2. Creation of a special template from all images of gray matter; processing of images of gray matter of the brain, correction, smoothing of structures and preliminary statistical analysis;
3. At the final stage, statistical processing of the prepared images is carried out, the result of which is the identification of areas of significant differences for qualitative assessment;
Resting functional connectivity analysis
Seed-based method is a hypothetical approach in which a certain region is selected as a reference, and temporal correlations between it and other brain regions are calculated. This method allows us to identify changes in functional connectivity that are characteristic of neuropsychiatric diseases.
As a reference (seed-region), the researchers chose both sides of the anterior cingulate cortex (ACC), since it is part of the limbic system. The limbic system is an important node of the emotional system, including the brain's default system and attention network, and has rich neural connections with the amygdala, thalamus and hippocampus. The ACC is also actively involved in the exchange of information with the prefrontal cortex (PFC). Selecting the anterior cingulate cortex as a region of interest (ROI) may be an important step in studying the mechanism of development of post-stroke depression. Whole-brain functional connectivity (FC) maps were generated separately for each patient group.
Disturbances of higher mental functions in massive lesions of the frontal lobes
Perceptual disturbances in frontal syndrome
Perception is designated as a complex perceptual activity that has a multicomponent composition, including the search for task-relevant elements of information, correlating them with each other, putting forward hypotheses, etc., that is, the process of perception presupposes the activity of the subject in the direction of solving a perceptual task. In patients with massive lesions of the frontal lobes, no noticeable disturbances in visual-perceptual activity are found when performing tasks for the perception and recognition of simple images, symbols, words, however, when performing sensitized (complicated) tasks that require active activity of the subject, difficulties are noted: adequate analysis of the presented stimuli is replaced by random, impulsive, influenced by immediate impressions, or formal responses that do not include an analysis of relevant information.
Movement and action disorders in frontal frontal syndrome
Since the departments included in the frontal lobes are responsible for maintaining tone, regulation, drawing up a motor program and control over ongoing activities, when they are damaged, disturbances in these functions are observed. Patients with massive lesions of the frontal lobes are unable to plan and carry out conscious, active actions. Moreover, speech instructions given from outside also lose their regulatory function. Patients with frontal syndrome not only have difficulty drawing up, but also cannot maintain a program of action, and either quickly replace it with uncontrolled, impulsive reactions, or demonstrate formed inert stereotypes of action, perseveratively repeating previously performed movements. The comparison of the result with the initially presented task is also impaired - such patients do not notice their mistakes. When the lesion is localized in the premotor parts of the frontal lobes, the patient demonstrates difficulties (even to the point of impossibility) in performing a series of movements: the “inhibition” of already completed stages of action and the smoothness of switching from one link of the kinetic program to another are disrupted, which in neuropsychology is defined as “the disintegration of the kinetic melody” .
Attention disturbances in frontal syndrome
The frontal lobes play a significant role in “inhibiting” reactions caused by the action of side stimuli and in the implementation of goal-directed, programmed behavior. Damage to the frontal lobes of the brain leads to impairments of voluntary attention, manifested in difficulties concentrating on a given instruction, the inability to inhibit reactions to external stimuli, impaired selectivity of mental processes, inactivity, distractibility, which interferes with the implementation of purposeful activities. Neuropsychological diagnostics of such a patient is effective in the case of his involuntary inclusion in a task, achieved within the clinic through interaction with the patient’s neighbor.
Memory impairment in frontal syndrome
With massive lesions of the frontal lobe, mnestic activity is disrupted: there are gross violations of the formation of intentions, planning, drawing up a behavior program, and the functions of regulation and control over the activities being carried out are disrupted. In patients with lesions of the convexital sections of the frontal lobes, the motive for active memorization is not formed, the memorization process turns into a passive imprinting of stimulus material: in the process of memorization, the memorization result does not improve, previously imprinted stimuli are stereotypically repeated. The learning curve in patients with such brain lesions has a characteristic plateau. In conditions of indirect memorization, such patients cannot correctly use auxiliary means, to the point that they not only do not improve memorization, but also worsen it, since they “distract” the patient during reproduction. With massive lesions of the frontal lobes, there is an increased inhibition of memory traces by interfering influence, which appears in the form of pathological inertia of previously emerged stereotypes. In other words, such patients have difficulty switching between tasks: when tasked with reproducing two groups of words, the patient inertly reproduces the group of words presented last. The same applies to memorizing material organized by meaning (sentences, stories, etc.). When the lesion is localized in the medial parts of the frontal lobes, in addition to the disorders described above, there are disturbances in orientation in the task and disturbances (up to the collapse) of the selectivity of mnestic processes. In such patients, severe disturbances of consciousness are often observed in combination with severe memory impairments.
Speech disturbances in frontal syndrome
In patients with massive damage to the frontal lobes of the brain, severe disturbances in active activity occur. Similar disturbances manifest themselves in the speech activity of such patients; they lack contact with people around them, based on their own initiative, while reactive speech behavior remains intact: they easily answer questions asked without grammatical defects in the structure of the statement. More complex forms of speech activity turn out to be inaccessible to patients with damage to the frontal lobes, since it turns out to be impossible to form complex motives and programs for speech utterance - speech aspontaneity appears. However, it is worth noting the fact that various phonetic, lexical, morphological and syntactic speech defects are absent, the apparatus of speech utterance remains intact, while extra-speech factors, such as instability of motives, disrupt the generation of speech utterance, which is replaced by uncontrolled associations and inert stereotypes, which must be minimized and filtering out connections that do not correspond to a given program and selecting only those that are suitable for the plan of speech utterance, a patient with a lesion given by localization cannot carry out.
Thinking disorders in frontal syndrome
Patients with massive damage to the frontal lobes retain the component elements of the task relatively well, but sometimes simplify (and the simplification is difficult to correct), or replace them, in accordance with inert stereotypes. Such patients find themselves practically unable to answer the question of a task, which is why the task loses its semantic structure, which is associated, according to A. R. Luria, with a violation of the predicative structure of speech and a violation of the dynamics of thinking. In patients with lesions of the frontal lobes, in most cases, there is a violation of the process of preliminary analysis and loss of the approximate basis of action. Without problems, they solve only those problems where the solution is clearly deduced from the conditions. If analysis (that is, orientation) and finding a solution program are required, they are not able to do this, but instead directly grab a fragment of the condition and immediately perform the operations. Pointing out an error to a patient with massive damage to the frontal lobes does not lead to its correction; moreover, the patient begins to pick out another fragment of the condition and perform operations corresponding to it. In such patients, there is also a violation of drawing up a plan for solving a problem. With frontal syndrome, there are also violations of systematic, hierarchically subordinated to the program, problem-solving operations. Patients with massive lesions of the frontal lobes either solve directly seized fragments of the problem using the same fragmentary operations, or use inert stereotypes formed when solving previous problems, or replace the solution with impulsive guesses, or even perform separate numerical operations, while completely distracting from the very meaning of the conditions of the problem, that is, they can begin to add kilograms with kilometers and so on. In the most severe cases of frontal syndrome, the disintegration of the action program is complemented by the inclusion of side effects that have no basis in the task conditions. Operations cease to be selective, and the intellectual process ceases to be organized. In addition, almost all patients with massive lesions of the frontal lobes, to a greater or lesser extent, demonstrate a defect in awareness of how their operations are proceeding - patients cannot tell how they came to this decision, they only name the last actions performed. Such patients are also unable to independently correct mistakes made.
Thus, we can conclude that the weakest link in the structure of mental activity in patients with frontal syndrome is the process of comparing the obtained result with the initial conditions of the task. This feature of patients with lesions of the frontal lobes is the most stable and is called “violation of criticism.” Summarizing the described characteristics of mental dysfunction in such patients, the defects observed in them can be reduced to violations of the functions of programming, regulation and control of mental activity.
Disorders of the emotional and personal sphere in frontal syndrome
Massive lesions of the frontal lobes almost inevitably entail a violation of the patient’s emotional and personal sphere. With frontal syndrome, all types of emotional phenomena are disrupted - emotional states, emotional responses and emotional-personal qualities, with the last, highest, personal level suffering the most. In general, the emotional-personal sphere in frontal syndrome is characterized by an inadequate (uncritical) attitude towards oneself, one’s condition, illness and others, and among the actual emotional manifestations the following are distinguished: states of euphoria, foolishness, emotional indifference, emotional dullness. With frontal syndrome, disturbances are observed in the spiritual sphere of a person - interest in work is lost, preferences in music, painting, etc. often change (or completely disappear), etc. At the same time, lesions in different parts of the frontal lobes entail different disorders. Thus, the most distinct disorders are observed in patients with damage to the mediobasal parts of the frontal lobes - such patients are characterized by disinhibition of primitive drives, impaired criticality, impulsivity, and affective disorders. With massive lesions of the convexital sections of the frontal lobes, disturbances in the emotional and personal sphere often manifest themselves in the form of apathy, indifference to oneself, one’s illness (anosognosia) and the environment, which occurs against the background of the general phenomena of adynamia and aspontaneity of mental functions, manifested in a given localization of the focal lesion. Interesting manifestations of interhemispheric asymmetry are observed with damage to the right or left frontal lobe: right-sided lesions are accompanied by uncriticality, motor and speech disinhibition, euphoria, sometimes even anger and aggressive manifestations; Left-sided lesions of the frontal lobes, on the contrary, are accompanied by general lethargy, lethargy, inactivity, depression, and depressive states.
This is a rather rough description of the syndrome of damage to the frontal lobes of the brain; in fact, the functional organization of the frontal lobes is heterogeneous: they include convexital (outer) and mediobasal (lower) sections, the functions of which are different, and, therefore, the syndromes that arise are different from each other when each of these departments is affected.
Frontal syndrome variants
In neuropsychology, various variants of frontal syndrome are distinguished.
Frontal syndrome with damage to the convexital parts of the frontal cortex of the brain
The convexital cortex is the outer portion of the frontal lobe and includes the premotor and prefrontal regions. In general, most of the characteristics of frontal syndrome relate specifically to damage to these parts of the frontal cortex. These departments form many bilateral connections with the cortical and subcortical structures of the brain, therefore, for example:
- Lesions of these departments, due to their close connection with the motor zone of the cerebral cortex, are accompanied by a violation of the organization of activity. In patients with lesions in the area of the premotor or prefrontal cortex, a breakdown of the motor program is detected, control over ongoing activities is impaired;
- When these areas of the cortex of the left (dominant) hemisphere of the brain are damaged, due to their connection with the cerebral organization of speech processes, there is disorganization of speech activity and the regulating, stimulating functions of speech, which manifests itself in the inactivity of speech processes, which makes it impossible for the patient to produce detailed statements. In general, this disorder of speech activity is known in neuropsychology as dynamic aphasia.
Separately, syndromes of damage to each of these parts of the frontal lobes are distinguished.
Premotor syndrome
It is characterized by the appearance of some motor awkwardness, which is based on a violation of the smoothness of “kinetic melodies”, which represent an automatic change of parts of a motor act. The violation of the smoothness of the execution of a motor act lies in the impossibility of inhibiting the action of the previous link and moving on to the next, in the inertia of one element of the action. For example, patients with this localization of brain damage are characterized by changes in handwriting, the automation of which disintegrates. Thus, in this syndrome, while the motivational component of the activity and the purposefulness of its course are preserved, the operational aspect of its implementation is disrupted.
Syndrome of damage to the areas of the cerebral cortex lying “anterior to the premotor zone”
This syndrome is intermediate between syndromes affecting the premotor and prefrontal zones. Within this syndrome, motor difficulties characteristic of premotor syndrome are not significantly expressed. Patients with this localization of the lesion are lethargic, aspontaneous, adynamic, inactive, experience difficulties in switching from one action to another, inertly get stuck on one level of activity, slip into a simplified version of the execution of the action, which manifests itself to a greater extent when performing intellectual tasks.
Prefrontal frontal syndrome
The central defect of this syndrome is a violation of the functions of programming, regulation and control and the motivational sphere, that is, the implementation of purposeful conscious activity, manifested in various mental functions, is disrupted. The main characteristics of the disintegration of goal-directed activity are: the absence of persistent motives, the regulating influence of a direct stimulus prevails over the regulating influence of verbal instructions, pathological inertia at the level of actions or programs, slipping into reinforced stereotypes, simplification of activity programs, violations of criticality and self-regulation of one’s own activities, lack of an internal picture of the disease .
Frontal syndrome with damage to the mediobasal parts of the frontal cortex
The medial and basal (deep) parts of the frontal lobes have a completely different functional organization. Lesions of the basal (orbital) parts of the frontal lobes, which are closely connected with the structures of the first block of the brain, the apparatus of the reticular formation and the structures included in the limbic system (the amygdala and other formations of the visceral brain) lead to a general disinhibition of mental processes and a gross change in affective processes . Lesions of the medial parts of the frontal lobes lead to a decrease in the tone of the frontal cortex and disruption of regulatory functions, states of wakefulness, which results in the appearance of such disorders as a decrease in the criticality and selectivity of mental processes. In addition, there are disturbances in orientation in space and time, instability of attention, gross memory impairment, confabulation, and confusion.
Basal frontal lobe syndrome
Data from clinical observations of patients with this localization of the lesion indicate the characteristic presence of disturbances in vision, smell and character, which manifests itself in disinhibition, affectivity, increased drives, decreased criticality and awareness of the difficulties experienced. The main neuropsychological factor of this syndrome is the pathological dynamics of the movement of mental processes, manifested in impulsivity, disinhibition and characteristic of all types of activity - gnostic, motor, mnestic, etc. A feature of this disorder is the impossibility of overcoming impulsivity by the regulatory influence of speech instructions with the possibility of assimilation and retention activity programs.
Syndrome of the medial frontal lobes of the brain
With sufficient preservation of praxis, speech, gnosis with the possible presence of impulsive but correctable reactions, patients with this localization of the lesion demonstrate disorientation in place and time, confabulation. A characteristic feature of such patients is the absence of doubts about the truth of their statements. The central defect in patients of this group is a violation of short-term memory and active retrieval of information after interfering influence, inactivity, impaired awareness of one’s own actions, and uncriticality.
Tumors located in the deep parts of the frontal lobes of the brain, involving the subcortical nodes, are manifested by a massive frontal syndrome, the central structure of which is a gross violation of goal-directed behavior (aspontaneity) and the replacement of relevant and adequate performance of activities with systemic perseverations and stereotypies.
In practice, when the deep parts of the frontal lobes are damaged, complete disorganization of mental activity is observed. The lack of spontaneity of patients is manifested by a gross violation of the motivational-need sphere. Compared to inactivity, where the initial stage of activity is still present and patients form an intention to complete a task under the influence of instructions or internal motivations, aspontaneity characterizes primarily a violation of the first, initial stage. Even the biological needs for food and water do not stimulate the spontaneous reactions of patients. Patients are untidy in bed, and the associated bodily discomfort also does not cause attempts to get rid of it. The “core” of the personality is broken, interests disappear. Against this background, the orienting reflex is disinhibited, which leads to a clearly expressed phenomenon of field behavior. The replacement of a conscious program of action with a well-established stereotype that has nothing to do with the main program is most typical for this group of patients.
In a clinical experimental study of these patients, despite the difficulties of interaction and cooperation with them, it is possible to objectify the process of the emergence of stereotypy. By the way, speaking here about stereotypies, we would like to emphasize their violent nature, the profound impossibility of inhibiting once actualized stereotypes. Their occurrence is based not only on pathological inertia, which is also observed with damage to the premotor area, but on the obvious stagnation, rigidity, and torpidity of those forms of activity that were able to be induced in the patient.
Deeply located processes in the frontal regions of the brain involve not only subcortical nodes, but also frontal-diencephalic connections, providing ascending and descending activating influences. Thus, in essence, with this localization of the pathological process, we have a complex set of pathological changes in the work of the brain, leading to pathology of such components of mental activity as goal setting, programming and control (the frontal cortex itself), tonic and dynamic organization of movements and actions (subcortical nodes) and energy supply of the brain, its regulation and activation (frontal-diencephalic connections with both vectors of activating influences).
It cannot be excluded that such a combination of structural and functional areas of damage and associated mental disorders simply does not leave intact areas in the nervous system with the help of which even minimal compensation of the defect would be possible, since the latter presupposes the presence of spontaneously regulated rearrangements or at least the preservation of the link adoption of external regulation of activities. A person’s cooperation with himself (L.S. Vygotsky) disintegrates, the patient becomes helpless. Only the sensory input remains open for interaction with the outside world when a stimulus that enters it directly causes habitual forms of activity. The latter, however, cannot adequately unfold and, in fact, embark on the path of multiple repetitions of themselves (perseveration and stereotypy).
It is characteristic that elementary perseverations that occur when the premotor-subcortical zone is damaged become especially pronounced in this syndrome. At the same time, so-called systemic perseverations arise as a forced reproduction of either a template for the method of an action performed once (in a study), or stereotyping the content of the latter. So, for example, A.R. Luria describes a patient who, after completing the action of writing and moving on to the task of drawing a triangle, draws it, but includes in the outline elements of writing the task. Another example of systemic perseverations is the inability to execute the instruction “two circles and a cross,” which is replaced by drawing a circle four times. The stereotype (“two circles”) that quickly forms at the beginning of execution turns out to be stronger than verbal instructions. The variety of systemic perseverations and their, paradoxically, complexity are most fully described by A.R. Luria in the book “Higher Cortical Functions of Man.”
Concluding the presentation of the main symptoms of damage to the deep parts of the frontal lobes of the brain, one cannot help but note the imaginary contradiction that may arise when perceiving the text between the aspontaneity syndrome described here and the data of a clinical experimental study that assumes the patient’s activity. As with other localizations of the pathological process, the severity of neuropsychological syndromes can be different, and the direction of influence of the tumor on the anterior or posterior parts of the frontal lobes changes the deficit in the voluntary regulation of functions. We should also not forget about the radical exhaustion of a function specific to a certain area of the brain, which is characteristic of all deep-seated tumors, with increasing load on the function, in particular, the duration of work within one system of actions. With regard to the syndrome of deep frontal tumors, this provision is important in the sense that both aspontaneity and gross perseverations can arise already in the process of working with the patient.
Impaired consciousness -previous|next- Hypothalamic-diencephalic region
N.K.Korsakova, L.I.Moskvichute. Clinical neuropsychology.
Literature
- Luria A.R. Higher human cortical functions and their disturbances in local brain lesions // 3rd ed. – M.: Academic Avenue, 2000. – 512 p..
- Luria A. R. Fundamentals of neuropsychology // M.: Academy, 2006..
- Luria A. R. Language and consciousness // Edited by E. D. Chomskaya. Publishing house Moscow. University, 1979. - 320 pp.
- Skvortsov A. A. Violations of programming, regulation and control of thinking with damage to the prefrontal parts of the brain // dissertation, Moscow, 2008.
- Luria A.R. Variants of “frontal syndrome” (to the formulation of the problem) // Pod general. ed. E.D. Chomsky, A.R. Luria. M.: Nauka, 1982..