Sjögren's syndrome - what is it? Causes, symptoms and treatment
Sjogren's syndrome (“dry syndrome”) is manifested by a decrease in the function of the exocrine glands; as a result of this pathology, severe dryness of the skin and mucous membrane of the vagina, trachea, nasopharynx, eyes, and oral cavity appears, and a decrease in the secretion of digestive enzymes produced by the pancreas is also observed.
Most often, this syndrome accompanies a number of autoimmune pathologies of connective tissue - dermatomyositis, scleroderma, and in such cases is called secondary Sjögren's syndrome. If the pathology develops independently, then the name sounds like primary Sjogren's syndrome, or Sjogren's disease.
Pathomorphology
The main morphological feature is the infiltration of the exocrine glands with lymph and plasma cells. First of all, the lacrimal and salivary glands are affected, a little less often – the glands of the bronchi, digestive tract and vagina.
- Both large and small glands are affected. At first, at an early stage of the disease, only small ducts are involved in the process; as it progresses, its infiltrate spreads further to the gland tissue itself, as a result of which the glandular tissue atrophies and is replaced by connective tissue. In some cases, the infiltrates described above occur not only in the exocrine (external secretion) glands, but also in other organs and systems of the body, in particular in the muscles, lungs and kidneys. This ultimately leads to dysfunction of the affected organ.
- In 30-40% of patients, in the material taken by biopsy of the salivary glands, metaplasia (modification) of the cells lining the ducts is determined: myoepithelial islands appear.
The lobules of the affected glands are destroyed in some patients, while in others the lobular structure is preserved. The glands are either enlarged in size or within normal limits.
Interestingly, even in the absence of clear clinical symptoms of Sjögren's syndrome, a patient with any connective tissue disease will most likely show histological signs of inflammation of the salivary glands.
Diagnosis of Sjögren's syndrome
The examination begins with examining the patient. The specialist should identify dry skin and tongue, the presence of ulcers on the oral mucosa and multiple caries, inflammation of the eyes and decreased tear production. Systemic damage to the connective tissue causes swelling of the parotid glands. Periodic swelling of the joints is possible, and upon palpation - pain. It is recommended to additionally listen to the lungs for wheezing.
When diagnosing Sjogren's syndrome, you need to consult a therapist, rheumatologist, ophthalmologist, dentist and other specialists. The dentist can clarify the nature of the damage to the salivary glands, excluding diseases with similar symptoms. An ophthalmologist performs a Schirmer test to assess the functionality of the tear glands: exposure to ammonia reduces the production of tear fluid. Marking of ocular structures makes it possible to identify erosion and dystrophy.
Laboratory tests to detect Sjögren's syndrome:
- General blood analysis. This syndrome is characterized by severe leukopenia, that is, a reduction in the number of leukocytes. Leukopenia indicates increased immune activity and the presence of anti-leukocyte antibodies. Almost all patients have mild or moderate anemia, and half have an increase in ESR. This is due to dysproteinemic disorders. An increase in CRP is not typical for Sjogren's syndrome (excluding effusion serositis, glomerulonephritis, destructive vasculitis, demyelinating neuropathy, intercurrent infection).
- General urine analysis. When Sjögren's disease is combined with urolithiasis or chronic pyelonephritis, the addition of a secondary infection causes leukocyturia (the presence of leukocytes in the urine). Characteristic signs of kidney damage include the presence of protein, glucose, red blood cells, casts in the urine, as well as a decrease in specific gravity and increased acidity of urine.
- Blood chemistry. There is a high concentration of γ-globulins, an excess of proteins, fibrin, sialic acids and seromucoid. Increased aminotransferase activity and cholestasis at an early stage of disease development may indicate concomitant viral or autoimmune hepatitis, cholangitis, liver or pancreas pathologies. If the total protein concentration increases and an M gradient is detected, additional diagnostics for plasma dyscrasias are necessary.
- Immunological reactions. Rheumatoid factor is detected in all patients, and its high titers indicate the presence of cryoglobulinemic vasculitis and the formation of MALT tissue. Cryoglobulins are detected in 1/3 of patients. Sjögren's syndrome is characterized by the following picture: an excess of IgG/IgA and IgM antibodies, the presence of antibodies to DNA, collagen and epithelium, the presence of lupus cells, an excess of B-lymphocytes and a lack of T-lymphocytes. Almost all have autoantibodies to nuclear antigens (Ro/SS-A and La/SS-B).
Unfavorable signs in Sjögren's syndrome include a decrease in complement C4, which signals the active development of cryoglobulinemic vasculitis. A sharp increase in the concentration of IgM immunoglobulins may indicate the concomitant development of lymphoma. If a patient has autoantibodies to thyroglobulin and thyroid peroxidase, it is necessary to diagnose autoimmune thyroiditis. In case of chronic liver dysfunction, tests reveal antimitochondrial antibodies, as well as antibodies to smooth muscles and microsomes (liver and kidney tissue).
Additional examination methods:
- sialography or contrast radiography;
- biopsy and ultrasound of the salivary glands;
- MRI of glands;
- X-rays of light;
- gastroscopy (checking the functioning of the esophagus and stomach);
- echocardiography (checking the functioning of the heart).
Ultrasound examination of the salivary glands makes it possible to assess their volume and structure, as well as identify inflammation, cysts and stones in the ducts. Magnetic resonance imaging provides the greatest amount of information about the functioning of the salivary glands. Chest X-rays are often uninformative. Computed tomography of the chest is effective only at an early stage of the disease, when the respiratory system is involved in the inflammatory process. Ultrasound examination of the abdominal organs can identify the causes of dry mouth and throat.
Patients with Sjögren's syndrome should visit a rheumatologist, ophthalmologist, and dentist regularly. It is advisable to see a gastroenterologist, since 80% of people with this disease also suffer from gastrointestinal disorders. At risk are people with a long history of Sjogren's disease and concomitant diffuse atrophic gastritis.
Reasons for development
The causes of Sjögren's syndrome have not yet been fully established. Among the most likely is the theory of a pathological reaction of the body's immune system. This reaction develops in response to damage to the cells of the external glands by a retrovirus, in particular the Epstein-Barr virus, herpes virus VI, cytomegalovirus, and human immunodeficiency virus. Despite the significant similarity of immunological disorders with changes in the body affected by the virus, direct evidence of the role of the virus as the cause of the development of pathology has not been obtained.
The viruses themselves and the epithelial cells of the glands changed by their influence are perceived by the immune system as antigens (foreign agents). The immune system produces antibodies against such cells and gradually causes the destruction of gland tissue. The disease often occurs as a hereditary or familial disorder, particularly among twins, suggesting that there is a genetic predisposition.
Thus, it is assumed that in the mechanism of development and occurrence of pathology, a combination of many factors is important:
- stress reaction of the body, which occurs as a result of the immune response;
- immune regulation with the participation of sex hormones, as evidenced by the rare incidence among people under 20 years of age, while girls are most often affected among children;
- immune control using T lymphocytes;
- viral;
- genetic.
There are two types of Sjögren's syndrome: primary, where symptoms of the disease are the first manifestations of it, and secondary, when symptoms appear in patients suffering from other rheumatic diseases, such as scleroderma, rheumatoid arthritis or systemic lupus erythematosus. Primary and secondary variants of the syndrome occur with approximately the same frequency. This sometimes makes it difficult to make an accurate diagnosis. Sjögren's syndrome is quite common: in the UK, for example, there are about half a million sufferers. Women aged 40 to 60 years are most often affected, while only one patient in 13 is male.
What is Sjögren's syndrome
Sjögren's disease or syndrome is an autoimmune disease that affects connective tissue in various body systems. The syndrome belongs to the group of collagenoses. These are the same type of functional and morphological changes in tissue, mainly in its collagen fibers. Collagenosis is characterized by constant progression and involvement of organs, structures of the musculoskeletal system, skin and blood vessels. Sjogren's disease is recognized as the most common among all collagenoses.
Most often, Sjogren's disease is detected in women 20-60 years old, although mainly after 40, when hormonal levels change due to menopause. The specific causes of autoimmune failure have not been clarified, but doctors identify hereditary predisposition and an aggressive response to infection as the most likely.
Symptoms of Sjögren's syndrome
Symptoms of the disease are divided into two groups:
- Glandular manifestations in which epithelial glands are affected and their functions are disrupted.
- Extraglandular manifestations. The symptoms of this group vary greatly, due to damage to various human organs.
Glandular symptoms include the following:
- Pathology of the lacrimal glands. In this case, unpleasant and painful sensations occur in the eyes (burning, as if the eyes are starting to sting, a sensation of sand in them), and characteristic itching and redness appear near the eyes. As a result, vision decreases, pinpoint hemorrhages, swelling, sensitivity to light, and eye pain occur.
- Pathology of the salivary glands. The manifestation of inflammation is mainly of the parotid glands, which are increased in size, sometimes with painful sensations. Dryness of the oral mucosa also occurs, swallowing food is difficult, often patients have to wash down food with water due to the problem of swallowing. In this case, the mucous membrane of the mouth takes on a bright pinkish tint.
- Dryness of the respiratory tract, which leads to inflammation of the bronchi, trachea, and lungs.
- Skin disorders resulting in dry skin.
- Damage to the nasal mucosa. The occurrence of dryness in the nose, covering with an intranasal crust, as a result of which inflammation develops.
Extraglandular manifestations are characterized by the following signs:
- The occurrence of tracheobronchitis, accompanied by cough and shortness of breath. It is not uncommon for a patient to be examined for pneumonia or pulmonary fibrosis.
- Enlarged lymph nodes.
- Damage to the peripheral nervous system. At the same time, painful sensations (tingling, burning) begin to appear.
- Fever;
- Pain in joints and muscles.
- Damage to the thyroid gland. It is a rare disorder in which allergic reactions to various foods, medications and other drugs begin to appear.
- Enlarged lymph nodes (submandibular, cervical, occipital). Enlargement of the liver and spleen is often observed.
- Inflammation of blood vessels, which occurs as a result of atherosclerosis of the lower extremities, due to circulatory disorders. When the functioning of blood vessels is disrupted, skin diseases (rashes) appear, which are accompanied by itching, burning and fever.
Often, against the background of the pathology we describe, patients develop increased individual sensitivity to certain drugs, in particular to non-steroidal anti-inflammatory drugs, some antibiotics (penicillin), so-called basic therapy drugs, and cytostatics.
Manifestations of Sjögren's disease
Symptoms of Sjogren's disease can be divided into glandular and extraglandular.
Glandular manifestations are caused by damage to the secreting glands, characterized mainly by a decrease in their function.
A constant sign of damage to the lacrimal glands in Sjögren's disease is eye damage associated with decreased secretion of tear fluid. Patients complain of burning sensations, “scratching” and “sand” in the eyes. Often there is itching of the eyelids, redness, and accumulation of viscous white discharge in the corners. Later, photophobia, narrowing of the palpebral fissures appear, and visual acuity decreases. Enlargement of the lacrimal glands in Sjögren's disease is rare.
The second mandatory and constant sign of Sjogren's disease is damage to the salivary glands with the development of chronic inflammation. It is characterized by dry mouth and enlarged salivary glands.
Often, even before the appearance of these signs, dryness of the red border of the lips, seizures, stomatitis, enlargement of nearby lymph nodes, and multiple (usually cervical) dental caries are noted. In a third of patients, a gradual enlargement of the parotid glands is observed, leading to a characteristic change in the oval of the face, described in the literature as a “hamster face” or “chipmunk face.”
In the initial stage of the disease, dry mouth appears only during physical activity and anxiety.
In the severe stage, dry mouth becomes constant, accompanied by the need to drink dry food and the desire to moisten the mouth during a conversation. The oral mucosa becomes bright pink and is easily injured. There is little free saliva, it is foamy or viscous. The tongue is dry. The lips are covered with crusts, inflammation is observed, and a secondary infection, including fungal and viral, may occur. Multiple cervical dental caries is characteristic.
The late stage is manifested by severe dryness of the mouth, the inability to speak, or swallow food without washing it down with liquid. The lips of such patients are dry, cracked, the oral mucosa shows signs of keratinization, the tongue is folded, and free saliva in the oral cavity is not detected.
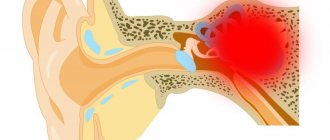
Dryness of the nasopharynx with the formation of dry crusts in the nose and in the lumen of the auditory tubes can lead to temporary deafness and the development of otitis media. Dryness of the pharynx and vocal cords causes hoarseness.
Frequent complications are secondary infections: sinusitis, recurrent tracheobronchitis and pneumonia. Damage to the glands of the external genitalia is observed in approximately 1/3 of patients with Sjogren's disease. The vaginal mucosa is reddened, dry, and patients are often bothered by burning pain and itching.
A common symptom of Sjögren's disease is dry skin. Sweating may be reduced.
Swallowing problems are caused by dry mucous membranes. Many patients develop chronic atrophic gastritis with severe secretory insufficiency, clinically manifested by heaviness and discomfort in the epigastric region after eating, belching of air, nausea, and loss of appetite. Pain in the epigastric region is less common.
There is a direct relationship between the degree of dryness and inhibition of the secretory function of the stomach. Damage to the bile ducts (cholecystitis) and liver (hepatitis) is observed in most patients. There are complaints of heaviness and pain in the right hypochondrium, bitterness in the mouth, nausea, and poor tolerance to fatty foods.
Involvement of the pancreas in the process (pancreatitis) is manifested by pain and digestive disorders.
Extraglandular manifestations of Sjögren's disease are very diverse and systemic in nature. Joint pain, slight stiffness in the morning. Signs of muscle inflammation (muscle pain, moderate muscle weakness, slight increase in the level of creatine phosphokinase in the blood) are observed in 5–10% of patients.
In most patients with Sjögren's disease, there is an increase in the submandibular, cervical, occipital, supraclavicular lymph nodes, and in 1/3 of patients the enlargement of the lymph nodes is widespread. In the latter case, liver enlargement is often detected.
Various respiratory tract lesions are observed in 50% of patients. Dry throat, soreness and scratching, dry cough and shortness of breath are the most common complaints.
In Sjögren's disease, vascular damage is observed. Pinpoint bloody rashes most often appear on the skin of the legs, but over time they spread higher and can be found on the skin of the thighs, buttocks and abdomen. The rash is accompanied by itching, painful burning and increased skin temperature in the affected area.
Damage to the nervous system with sensory disturbances of the “socks” and “gloves” type, neuritis of the facial and trigeminal nerves are observed in a third of patients.
A third of patients experience allergic reactions, more often to antibiotics, sulfonamides, novocaine, group B drugs, as well as to chemicals (washing powders, etc.) and food products.
Diagnostics
Burning eyes and dry mouth may not always mean that a person has this syndrome. Sjögren's syndrome can be diagnosed only in the presence of inflammatory lesions of the glands. However, there are cases when various metabolic diseases can lead to a similar result, in which the secretion of saliva is significantly reduced (most often this is diabetes mellitus).
As a result, the functions of the salivary and lacrimal glands prematurely decline in older people. These forms of dry eyes and dry mouth have nothing to do with Sjögren's syndrome. Tissue examination is also performed to diagnose this syndrome. For this type of study, small fragments of the oral mucosa are taken, which are examined using a microscope. In this way, damage to the mucous glands is established.
3. Symptoms and diagnosis
It is not for nothing that Sjögren’s disease is called “dry syndrome”: the classic picture of Sjögren’s disease includes two obligate symptoms that are mandatory for diagnosis - xerophthalmia (dry eyes) and xerostomia (dry mouth); For a secondary syndrome, the presence of another, previously manifested systemic connective tissue disease is required.
Insufficient hydration of the eyeballs, caused by lymphoid infiltration of the lacrimal glands, leads to the development of dry keratoconjunctivitis (inflammation of the cornea and conjunctiva, sometimes ulcerative) with corresponding symptoms.
Constant drying out of the oral mucosa causes a number of serious dental disorders and leads to problems with food consumption.
Optional symptoms are very diverse: photosensitivity (pathological hypersensitivity of the skin to sunlight) with an erythematous rash in open areas, joint-muscular pain and swelling, cheilitis (inflammation and cracks on the lips and in the corners of the mouth), gastrointestinal disorders, sexual dysfunction in women (since not only salivary and lacrimal glands are affected, but also other exocrine glands, including those responsible for moisturizing the vagina), allergic reactions, dry bronchitis and other respiratory diseases, renal pathology, vasculitis (inflammation of blood vessels), damage to the central nervous system and etc. The most dangerous complications of Sjogren's disease/syndrome include oncological processes (usually lymphomas or lymphosarcoma), the likelihood of which increases by more than 40 times with this disease.
Diagnosis is based on the results of studying the anamnesis, clinical picture and dynamics, as well as on data from ophthalmological, dental, oncological, and endocrinological examinations. Additionally, imaging diagnostic methods and biopsy of affected tissues are prescribed. However, a multifaceted laboratory blood test is critical.
About our clinic Chistye Prudy metro station Medintercom page!
Complications
Common consequences of Sjögren's syndrome:
- lymphomas (neoplasms affecting the blood and lymph nodes);
- vasculitis (an inflammatory process in blood vessels that can occur everywhere);
- addition of a secondary infection;
- development of cancer;
- inhibition of blood formation, reduction in the blood of leukocytes, erythrocytes and/or platelets.
If the patient does not take any measures to treat Sjögren’s disease for a long time or he was prescribed the wrong therapy, the pathology progresses, leading to serious disruptions in the functioning of organs and systems.
Symptoms
In Sjögren's disease, symptoms can be divided into two groups. The first includes symptoms associated with the functioning of the glands, and the second includes symptoms manifested in other organs and systems of the body.
Symptoms that appear when the salivary glands are involved:
- inflammation of the salivary glands near the ear area, accompanied by pain and changes in their size;
- due to the lack of saliva, the oral cavity dries out and it is difficult to swallow food;
- the oral cavity takes on a bright pink color and is easily injured;
- due to the almost complete absence of saliva, the tongue is constantly dry, and a dry crust appears on the lips;
- caries appears on the teeth.
Symptoms that occur when the lacrimal glands are damaged:
- burning in the eyes, feeling of “sand” and itching;
- redness of the eyelids;
- painful sensations in bright light;
- decreased visual acuity;
- the formation of purulent ulcers on the cornea of the eye.
Symptoms that appear when other glands are affected:
- dryness in the nasopharynx;
- hearing loss due to inflammation;
- due to dryness in the vocal cords, the voice becomes hoarse;
- due to dryness in the respiratory tract, diseases such as bronchitis or pneumonia may occur;
- when the external genital organs are affected, itching and severe pain often occur;
- sweat secretion decreases;
- Due to dryness, cracks and peeling often occur on the skin.
Symptoms that appear when the disease spreads to internal organs:
- increased body temperature;
- painful sensations in the joints without signs of inflammation;
- pain in muscle tissue;
- damage to the gastrointestinal tract - gastritis, inflammation of the pancreas and biliary system, which is characterized by attacks of nausea, vomiting, abdominal pain;
- inflammatory lesions of blood vessels, which may result in a skin rash and ulcers. When the blood vessels on the fingers are damaged, the blood flow is disrupted, the fingers change color, and painful sensations appear;
- an inflammatory process may occur in the kidneys leading to renal failure;
- possible enlargement of lymph nodes;
- if the lungs are damaged, a constant dry cough occurs;
- if the thyroid gland is damaged, it may become enlarged and malfunction;
- Allergic reactions to medications often occur.
Treatment of Sjögren's syndrome
In the presence of Sjögren's syndrome, treatment is carried out depending on the stage of the disease and the presence of systemic manifestations.
In order to stimulate the function of the glands, the following is carried out:
- drip administration of contrical.
- subcutaneous administration of galantamine.
- Vitamin therapy courses are conducted for general strengthening purposes.
- As a symptomatic treatment, “artificial tears” (drops in the eyes) are prescribed - with low viscosity - Lakrisifi (200-250 rubles), Natural Tear (250 rubles), medium viscosity Lakrisin, high viscosity Oftagel 180 rubles, Vidisik 200 rubles, Lacropos 150 rubles .
At the initial stages, in the absence of damage to other systems and unexpressed laboratory changes, long courses of glucocorticosteroids (prednisolone, dexamethasone) in small doses are prescribed.
If symptoms and laboratory parameters are significantly pronounced, but there are no systemic manifestations, cytostatic immunosuppressive drugs - cyclophosphamide, chlorbutin, azathioprine - are added to corticosteroids. Maintenance therapy is carried out with the same drugs for several years.
- If there are symptoms of systemic damage, regardless of the stage of the disease, high doses of corticosteroids and immunosuppressants are immediately prescribed for several days with a gradual transfer to maintenance doses.
- For generalized polyneuritis, vasculitis, kidney damage and other severe manifestations of the disease, the following methods are added to the above treatment, extracorporeal treatment - plasmapheresis, hemosorption, plasma ultrafiltration.
- The remaining drugs are prescribed depending on complications and concomitant diseases - cholecystitis, gastritis, pneumonia, endocervicitis, etc.
In certain cases, it is necessary to follow a dietary diet and limit physical activity.
Treatment of Sjögren's disease
The main place in the treatment of Sjogren's disease belongs to hormones and cytostatic immunosuppressants (chlorbutin, cyclophosphamide).
In the initial stage of the disease, in the absence of signs of systemic manifestations and moderate abnormalities in laboratory parameters, long-term treatment with prednisolone in small doses (5–10 mg/day) is advisable.
In severe and late stages of Sjögren's disease, in the absence of signs of systemic manifestations, it is necessary to prescribe prednisolone (5–10 mg/day) and chlorobutine (2–4 mg/day), followed by long-term, for several years, maintenance doses of prednisolone (5 mg/day). day) and chlorbutin (6–14 mg/week).
This regimen can be used to treat patients in the initial stages of the disease in the presence of severe disturbances in laboratory indicators of process activity, as well as cryoglobulinemia without clear signs of systemic manifestations.
Pulse therapy with high doses of prednisolone and cyclophosphamide (1000 mg of 6-methylprednisolone intravenously daily for three days in a row and a single intravenous injection of 1000 mg of cyclophosphamide), followed by transfer to moderate doses of prednisolone (30–40 mg/day) and cytostatics (chlorobutin 4- 6 mg/day or cyclophosphamide 200 mg intramuscularly 1–2 times a week) in the absence of effects on the liver is the most effective treatment for patients with severe systemic manifestations of Sjögren's disease, is generally well tolerated by patients and avoids many of the complications associated with long-term use high doses of prednisolone and cytostatics.
Extracorporeal treatment methods (hemosorption, cryoadsorption, plasmapheresis, double plasma filtration) in combination with pulse therapy are most effective in the treatment of patients with Sjögren's disease with ulcerative necrotizing vasculitis, glomerulonephritis, polyneuritis, myelopolyradiculoneuritis, cerebrovasculitis caused by cryoglobulinemia.
Local therapy for eye damage is aimed at eliminating dryness and preventing secondary infection. Dry eyes are an indication for the use of artificial tears. The frequency of use of drugs depends on the severity of damage to the organ of vision and ranges from 3 to 10 times a day.
To protect the cornea, therapeutic soft contact lenses are used. To prevent secondary infection, use solutions of furatsilin (at a dilution of 1:5000), 0.25% solution of chloramphenicol, ciprofloxacin, etc.
Therapy for chronic inflammation of the salivary glands is aimed at overcoming dryness, strengthening the walls of the salivary gland ducts, preventing exacerbations, improving the restoration of the epithelium of the oral mucosa and fighting secondary infections.
In order to normalize nutrition and secretion of the salivary glands, novocaine blockades are used. In cases of exacerbation of chronic parotitis (and to prevent its relapses), applications of a 10–30% dimexide solution are used. In cases of the development of purulent parotitis, antibiotics are injected into the ducts of the salivary glands and antifungal drugs (nystatin, levorin, nystatin ointment) are prescribed locally. To reduce the permeability of the ducts, calcium preparations are administered intravenously or intramuscularly.
It is possible to accelerate the healing of the mucous membrane of the oral cavity and the red border of the lips when erosions and cracks occur with the help of rosehip and sea buckthorn oils, solcoseryl and methyluracil ointments, as well as by treating the oral mucosa with ENKAD (active nucleic acid derivatives). Decamine caramel also has antibacterial properties.
For dry nasal mucosa, frequent applications of isotonic sodium chloride solution are used (using turundas).
Vaginal dryness is reduced by using potassium iodide jelly.
For dry trachea and bronchi, long-term use of bromhexine is recommended (8–16 mg 3 times a day for 2–3 months).
If there are signs of chronic gastritis with secretory insufficiency, replacement therapy is carried out for a long time (hydrochloric acid, natural gastric juice, pepsidil).
Pancreatic insufficiency requires taking enzymes: Panzinorm, Creon, Festal in courses of 2-3 months or continuously, treatment is also carried out with solcoseryl (2 ml intramuscularly 2 times a day for 15-30 days).
Forecast
Sjögren's syndrome can damage vital organs with a transition to a stable state, gradual progression, or, conversely, long-term remission. This behavior is also typical for other autoimmune diseases.
- Some patients may have mild symptoms of dry eyes and mouth, while others develop serious complications. Some patients are completely helped by symptomatic treatment, others have to constantly struggle with deterioration of vision, constant discomfort in the eyes, often recurrent infections of the oral cavity, swelling of the parotid salivary gland, difficulty chewing and swallowing. Constant loss of strength and joint pain seriously reduce the quality of life. In some patients, the pathological process involves the kidneys - glomerulonephritis, leading to proteinuria, impaired renal concentrating ability and distal renal tubular acidosis.
- People with Sjögren's syndrome have a higher risk of developing non-Hodgkin's lymphoma compared to healthy people and people with other autoimmune diseases. About 5% of patients develop some form of lymphoma.
In addition, it has been found that children of women with Sjogren's syndrome during pregnancy have a higher risk of developing neonatal lupus erythematosus with congenital heart block.
Causes of Sjögren's syndrome
The cause of Sjögren's syndrome is not yet entirely understood. The presence of activated salivary gland epithelial cells expressing major histocompatibility complex (MHC) class II molecules and the identification of inherited markers of susceptibility suggest that environmental or endogenous antigens trigger the inflammatory response in susceptible individuals.
Association with human leukocyte antigen
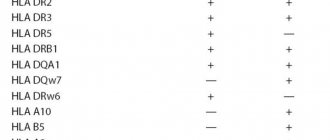
The frequency of the presence of the HLA-DR52 autoantigen in patients with primary SS is estimated at 87%, but it is also significantly increased in secondary Sjögren's syndrome.
Genetic associations for Sjögren's syndrome vary among ethnic groups. For example, in Europeans this condition is associated with human leukocyte antigens (HLA)-DR3, HLA-DQ2, HLA-B8, while in Hispanics it is associated with HLA-DR5.
Some evidence suggests that the true association of Sjögren's syndrome may be with HLA-DQA1, which is in linkage disequilibrium with HLA-DR3 and HLA-DR5.
Possible triggers of the disease
Viruses are considered good candidates for environmental triggers, although no proof of causation has yet been provided.
Damage or death of cells due to viral infection or other causes can trigger antigens to Toll-like receptors on dendritic or epithelial cells, which, when activated, begin to produce cytokines and chemokines.
Sex hormones
Sex hormones may influence the immunological manifestations of primary Sjögren's syndrome because the disease occurs much more often in women than in men. The prevalence of serological markers is generally lower in male patients than in female patients. Although the role of sex hormones (eg, estrogens, androgens) in the pathogenesis of primary SS remains unknown, deficiency of adrenal and gonadal steroid hormones likely affects immune function.