What is a basal skull fracture?
A basal skull fracture is a very severe traumatic brain injury (TBI) in which one or more of the bones that make up the base of the skull: the occipital, sphenoid, temporal or ethmoid, breaks. The cause of such damage is usually a significant impact: it could be an accident, a fall backward from a height, a direct blow from something heavy to the head or face in the lower jaw area.
Fracture of the bones of the base of the skull accounts for 4% of the number of diagnosed traumatic brain injuries. A combination of fractures of the base and vault of the skull is also possible, which occurs in 50-60% of patients with this injury.
Survival rate for skull fracture
Of decisive importance is how quickly and competently first aid is provided for a fracture and hospitalization with subsequent medical measures is carried out. TBI is often accompanied by heavy bleeding, which can lead to death in the first hours after injury or cause a prolonged coma, the prognosis of which is extremely unfavorable. In this case, there is a high probability of lifelong disability, when basic life functions are impaired and intelligence is seriously affected.
For fractures without displacement, single cracks that do not require surgical intervention, the prognosis is relatively favorable.
The mortality rate for fractures of the bones of the base of the skull ranges from 24 to 52%, depending on the severity and complexity of the injury and its subsequent complications.
Causes of such injuries
Skull fractures occur as a result of the application of great force. They most often affect young and middle-aged people who lead an active life or play sports. As well as alcoholics, drug addicts and representatives of criminal structures. There are several reasons why skull fractures occur:
- strong blows to the head with a hard object;
- falling from a height;
- car crashes;
- gunshot wound.
There are two mechanisms for obtaining such an injury: direct and indirect. When a bone breaks where force is applied, it is a direct fracture. This is how cranial vault injuries usually occur. Damaged bones are often pressed inward and damage the meninges. With an indirect fracture, the impact is transferred from other bones. For example, when falling from a height onto the pelvis or legs, a strong blow is transmitted through the spine to the base of the skull, often leading to a fracture.
Signs and symptoms of a skull fracture
Symptoms depend on the severity, location of the fracture, and the extent of damage to brain structures. Loss of consciousness can take any form, from short-term fainting at the time of injury to long-term coma. The more severe the damage, the more severe the damage, but with intracranial hematoma there may be a period of lucidity preceding loss of consciousness, which should not be mistaken for the absence or mildness of injury.
Common signs of a fracture include:
- Expanding headaches due to developing cerebral edema;
- Vomiting, aspiration of vomit, or spontaneous leakage of stomach contents into the lungs;
- Symmetrical bilateral hemorrhages around the eyes in the form of “spectacles”;
- Different diameters and lack of pupillary response;
- Respiratory and circulatory disorders in case of compression of the brain stem;
- Leakage of cerebrospinal fluid (cerebrospinal fluid), mixed with blood, from the nose and (or) ears;
- Cardiac disorders: arrhythmia, tachycardia, bradycardia, high or low blood pressure;
- Excitement or immobility;
- Confusion;
- Involuntary urination.
Fractures of the temporal bone pyramid can be longitudinal, transverse, or diagonal. With longitudinal fractures, the middle and inner ear and the facial nerve canal are affected. Symptoms: bleeding from the ear and leakage of cerebrospinal fluid due to a ruptured eardrum, hemorrhage in the area of the temporal muscle and behind the ear, partial hearing loss. Bleeding increases when you turn your head, so this is strictly prohibited.
A transverse fracture of the temporal bone is characterized by complete loss of hearing, disturbances in the functioning of the vestibular apparatus, paralysis of the facial nerve, and loss of taste.
- Clinical signs of anterior fossa fracture: nosebleeds, nasal liquorrhea (cerebrospinal fluid discharge through the nose), hemorrhages around the orbits and under the conjunctiva. Bruises appear 2-3 days after the injury, which fundamentally distinguishes them from ordinary bruises that appear as a result of direct blows to the face. Sometimes so-called subcutaneous emphysema occurs: when the cells of the ethmoid bone are damaged, air penetrates into the subcutaneous tissue, causing blisters to form on the skin.
- Clinical signs of a middle cranial fossa fracture: unilateral ear bleeding; a sharp decrease in hearing or complete deafness; release of cerebrospinal fluid due to a ruptured eardrum, dysfunction of the facial nerve, bruising in the area of the temporal muscle and behind the ear; partial loss of taste. Middle fossa fractures account for 70% of skull base injuries.
- Clinical signs of a fracture of the posterior cranial fossa: simultaneous damage to the auditory, facial and abducens nerves; bruising behind the ears on one or both sides; when the caudal nerves are pinched or ruptured, the tongue, palate, and larynx are paralyzed and the functioning of vital organs is disrupted.
- Fractures of the base of the skull are also characterized by damage to the olfactory or optic nerve. With such fractures, the meninges are ruptured, as a result of which a communication channel is formed between the brain matter and the external environment through the nasal and oral cavities, middle ear or orbit. Splinter fractures are especially dangerous in this regard: bone fragments can injure arteries and veins. Communication with the external environment leaves the brain open to infections and microbes and can lead to the development of encephalitis, meningitis or brain abscess.
The consequences of such injuries
If the skull fracture is linear, without displacement of bones or large hematomas, and also if purulent infection has been avoided, then the prognosis for recovery is usually favorable. But a skull fracture does not always go away without complications. The consequences of such an injury can be very serious:
- meningitis, encephalitis;
- intracerebral hematomas can lead to encephalopathy;
- excessive bleeding most often ends in death;
- after a comminuted fracture of the base of the skull, paralysis of the entire body may develop;
- Patients often suffer from psychological and emotional disorders and decreased mental abilities.
First aid for a skull fracture
If you suspect a fracture, you should immediately call an ambulance. If the victim’s condition is satisfactory and he is conscious, then he should be placed on his back (without a pillow), his head and upper body immobilized and secured, and an antiseptic bandage applied to the wound. If hospitalization is delayed, dry ice can be applied to the head. If there are no breathing problems, you can give the victim diphenhydramine or analgin.
In an unconscious state, the victim should be laid on his back in a half-turn position and his head should be turned slightly to the side to avoid aspiration in case of vomiting, loosen tight clothes, remove existing glasses, dentures, and jewelry. To secure the body, place a cushion of clothing or a blanket under one side of the body.
In case of acute respiratory distress, artificial respiration is performed through a mask. Cardiovascular drugs (sulfocamphocaine, cordiamine), glucose solution, Lasix are administered. In case of heavy bleeding and a sharp drop in pressure, Lasix is replaced with intravenous administration of polyglucin or gelatinol. During motor excitation, a solution of suprastin is injected intramuscularly.
Painkillers should be used with caution as they may complicate bleeding. The use of narcotic painkillers is contraindicated; they aggravate respiratory disorders.
Classification of skull base fractures
Fractures vary:
- According to the damaged bones of the same name;
- Along the cranial fossae of the inner surface of the skull: anterior, middle and posterior;
- In relation to the external environment;
- By the presence or absence of bone displacement.
The occipital and sphenoid bones are part of the brain section of the skull. The temporal bones form the cranial vault and house the hearing organs: the pyramid of the temporal bone contains the tympanic cavity and the inner ear. The anterior fossa is formed by the frontal bone, the plate of the ethmoid bone, and is separated from the middle fossa by the edges of the sphenoid bone. The middle fossa is formed by the sphenoid and temporal bones. The posterior fossa is formed by the occipital bone, the posterior part of the sphenoid bone.
Non-displaced fractures are classified as open TBIs and have a favorable prognosis. If the fracture is accompanied by blood loss or leakage of cerebrospinal fluid, it is considered an open penetrating type TBI.
Types of damage
The classification of skull fractures is based on various signs.
Table 1. Various injuries to the base of the skull:
| Type of fracture | What does it look like |
| Without displacement of fragments - a simple fracture of the base of the skull and bones of the cranial vault. |
|
| With displacement of fragments - a complex fracture. |
|
| Without pressing bones into the cranial cavity. | Fracture without depression |
| With depression of bones into the cranial cavity and damage to the brain. |
|
| Linear bone fracture. |
|
| Serrated bone fracture. | The fracture line is zigzag |
What happens when the base of the skull is fractured? The bones of the skull contain cavities filled with air. Damage to them leads to the release of air into the soft tissues of the head. Almost always there is a violation of the integrity of the periosteum. As a result, all cavities and openings of the skull can communicate with each other.
Fractures of the base of the skull and temporal bone, as well as the occipital bone, are often accompanied by the formation of fragments and brain damage. It should be remembered that there are two bones that are located inside the skull and during an external examination their fracture may not be detected - the ethmoid and the sphenoid. Therefore, any head impact should first be considered a potential skull fracture.
Treatment of a skull fracture
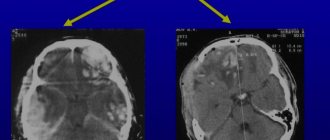
For an accurate and detailed diagnosis of injury, magnetic resonance imaging (MRI) or computed tomography (CT) is used. Depending on the severity and complexity of the damage, treatment can be conservative or surgical.
Conservative treatment
Conservative methods are indicated for mild to moderate injuries, when liquorrhea can be eliminated non-surgically.
It is necessary to observe strict bed rest, the head should be in an elevated position - this helps to reduce the secretion of cerebrospinal fluid. Treatment includes dehydration therapy (aimed at reducing fluid content in the organs), for this purpose, lumbar punctures (taking cerebrospinal fluid from the spinal cord at the lumbar level) are performed every 2-3 days, and subarachnoid insufflations (introduction into the subarachnoid space of the spinal cord) are carried out in parallel. the same amount of oxygen. Drugs that reduce the production of cerebrospinal fluid are also used - diuretics Diacarb, Lasix.
Physical activity is limited for six months. The victim must be registered with a traumatologist and neurologist, and be observed by an otolaryngologist and an ophthalmologist.
Particular attention should be paid to the prevention of intracranial complications of a purulent nature. For this purpose, sanitation of the nasopharynx, oral cavity and middle ear is carried out using antibiotics. In the presence of purulent complications, intramuscular or intravenous injections are supplemented by the introduction of antibiotics into the epidural space (endolumbar). For this, kanamycin, chloramphenicol, monomycin, and polymyxin are used. Also, endolumbar administration of kanamycin is carried out 2 days after the cessation of liquorrhea. The best way to select a drug is by culture of the cerebrospinal fluid flora or a smear taken from the nasal mucosa.
Surgery
Surgery is necessary in the following cases:
- Detection of a comminuted fracture;
- Damage or compression of brain structures;
- Leakage of cerebrospinal fluid through the nose, which cannot be stopped by conservative methods;
- Recurrences of purulent complications.
Surgical treatment is used in the presence of bleeding, hematoma or bone fragments that may pose a direct threat to life. In this case, trephination (opening) of the skull is performed, and after the operation, the bone tissue defect is closed with the removed bone or a special plate (in most cases). This is followed by long-term rehabilitation.
On topic: 12 folk methods for home treatment
Diagnosis of injuries
For any traumatic brain injury, an examination is performed to rule out a fracture. In addition to questioning the victim or his accompanying persons about the circumstances of the injury, the doctor examines the patient. Sensitivity, the presence of reflexes are assessed, the pulse and the reaction of the pupils to light are checked. An X-ray of the skull is also taken in two projections. To confirm the diagnosis, the results of magnetic resonance and computed tomography, brain puncture and echoencephalography are used. Such a study must be carried out even in the absence of visible consequences of injury, since after an impact only the inner plate of the skull bones can be damaged.