Types and classification
Symptoms of agnosia vary significantly depending on the damaged area of the cerebral cortex. Most often, one type of perception is affected, but the disease can affect several systems simultaneously. There are several main types of agnosia:
- visual (visual);
- auditory;
- olfactory - impaired perception of smells;
- tactile - change in response to touch;
- taste;
- other specific varieties.
Specialists at the Clinical Brain Institute have extensive experience working with patients with agnosia. It is important to promptly determine the type of disorder and begin maintenance therapy. In addition, the first signs of the disease may indicate serious pathologies of nervous activity.
Visual agnosia
This type of agnosia is characterized by a violation of the perception of information that enters the brain through the visual analyzer. Its symptoms may differ for each patient, depending on the type and location of the damage. So, we can distinguish several specific varieties:
- object-based (develops when the left occipital lobe is damaged) - the patient sees objects well, but has difficulty recognizing them;
- prozolagnosia (damage to the lower occipital region on the right) - inability to recognize even familiar faces;
- color (damage in the left occipital region) - difficulty identifying colors and shades, as well as determining their relationship with certain objects;
- weakness of optical representations (symmetrical damage to the occipital-parietal lobe) - inability to determine the color, shape and size of objects, imagine and describe them;
- simultaneous (pathology of the occipital region) - the patient can concentrate on only one object;
- Balint's syndrome (damage to the occipito-parietal region) - inability to direct the gaze and focus on objects that are in different directions, as well as difficulty identifying objects at near and far distances.
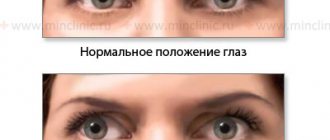
With visual agnosia, the normal functioning of the other sense organs is maintained, and no eye diseases are detected. After rehabilitation at the Clinical Institute of the Brain, the patient adapts to everyday life and can compensate for visual disorders using other analyzer systems.
Optical and optical-spatial agnosias
Patients experience impaired ability to determine the distance between objects and navigate in space. In this category, several specific types of agnosia can be distinguished:
- Depth agnosia (damage to the middle part of the occipital-parietal lobe) - difficulty determining the distance to objects, especially those located in the anterior direction from the patient;
- impaired stereoscopic vision (pathology in the left hemisphere) - inability to recreate a three-dimensional image;
- unilateral (damage to the opposite parietal region) - one half of the space falls out of the field of vision;
- Topographical orientation disorder (parietal and occipital regions) - difficulty finding familiar objects, including home address and objects in one’s own home.
Memory and attention are preserved in optical-spatial agnosia. The patient will need help with everyday life and with new tasks, but proper rehabilitation will allow him to experience minimal discomfort in everyday life.
Auditory agnosia
With this type of agnosia, the functions of the auditory analyzer are preserved. The patient may experience various auditory perception disorders, including:
- simple - decreased ability to characterize and identify familiar sounds;
- auditory-speech - impaired speech recognition, recognition of simple and familiar words;
- tonal - lack of understanding of voice timbre, emotional coloring and other aspects.
All types of auditory agnosia develop when the temporal lobe of the brain is damaged. If the patient is unable to recognize speech, he experiences difficulties in everyday life, while his memory, attention, and the functions of the visual and other analyzers compensate for the impairment.
Somatoagnosia
Somatoagnosia is a disorder in which the patient is unable to identify and recognize parts of his own body. These are complex perception disorders associated with damage to various parts of the right hemisphere of the brain. There are two main types of somatoagnosia:
- Anosognosia is a condition in which the patient denies the presence of an illness. This may be ignoring paralysis of limbs, blindness, or speech disorders.
- Autotopagnosia is a disorder of the ability to recognize individual parts of the body. The patient experiences difficulty when asked to point to an arm, leg, or face; in some cases, there is a feeling of a change in the size of parts of the body. This group also includes somatic allosthesia, in which the patient experiences a feeling of an increase in the number of limbs.
Signs of somatoagnosia may occur in attacks. Thus, in some patients they are harbingers of an epileptic attack, and with proper treatment they are practically invisible and do not cause inconvenience in everyday life. However, they can persist permanently.
Impaired awareness of space and time
This type is considered the rarest and is associated with damage to the occipital lobe of the cerebral cortex. The patient has difficulty determining the passage of time, as well as the speed of movement of any objects. Separately, there is akinetopsia - impaired ability to identify moving objects.
Optical-spatial agnosia and its types
Agnosia is said to occur when a person’s perception (visual, auditory, tactile) is impaired due to damage to the cerebral cortex, but at the same time clear consciousness and normal sensitivity are maintained.
With damage to the superior parietal and parieto-occipital areas of the cortex of both the right and left hemispheres, optical-spatial agnosia . It is in these zones that the visual, auditory, tactile and vestibular systems interact in a complex manner. The manifestations of optical-spatial agnosia are especially noticeable with bilateral lesions, but even with a lesion on one side, the disturbances are clear.
Kasperovich Anna
A person with optical-spatial agnosia cannot navigate in space (even in his own home), find a well-known road and return home. He cannot recognize the spatial characteristics of the objects that he sees, that is, he does not understand their three-dimensional model, namely the size and depth of the object, its distance (distance to the object), direction and location in relation to other objects (for example, he does not see which the object is lower and further, higher and closer), confuses right and left, top and bottom. He is not always able to count the number of objects (real and in the picture). Difficulties are also caused by determining the cardinal directions, understanding the coordinates of the area, determining one’s location on a geographic map, and a schematic representation of one’s house (room, apartment). Sometimes orientation in real (three-dimensional) space is not affected, but there are violations on paper (in two-dimensional space).
Fernando Vicente
With a lesion (or dysfunction) on the left , orientation in space (namely, schematic representations) is disrupted, that is, a person cannot mentally rotate a geometric figure in space, is not able to navigate a geographical map, a watch dial, etc. His ability to draw suffers, since he cannot convey important spatial characteristics, that is, to depict one object further or closer, larger or smaller than another, and he also cannot navigate the sides (right and left) and the pattern of the drawing (top and bottom). Sometimes the patient is unable to connect the individual parts of one object, he depicts them separately from each other (for example, when drawing a kitten, the result is not an animal, but a set of its body parts - ears, tail, paws, etc.). Despite this, the patient can still copy the drawn image. In a person with optical-spatial agnosia, the body diagram is disrupted (see Autotopagnosia), and finger agnosia also appears, when the patient cannot identify and name the fingers that are touched or pointed at.
Also, a person with optical-spatial agnosia does not understand and cannot name words with a spatial meaning (prepositions: on, under, for, above, in, etc.; adverbs: close, on the side, on top, etc.), which is why his speech is often becomes agrammatic, similar to the speech of people with semantic aphasia. In addition, with left-sided optical-spatial agnosia, reading and written speech suffer, because the simultaneous performance of actions and sound-letter analysis of words are difficult. As a rule, asymmetrical letters cause difficulties, that is, those whose right and left sides differ from each other (p, k, h, i, etc.).
An example of a technique for determining difficulties in understanding spatial prepositions from Luria’s neuropsychological album
With a lesion (or dysfunction) on the right , insufficient holistic perception of the situation and simultaneous agnosia are observed (a person cannot describe a plot picture, since he does not perceive the image as a whole, but in pieces, separate fragments, but at the same time he often recognizes individual objects and people).
An example of a plot picture from Luria’s neuropsychological album
Autotopagnosia is also observed; the patient cannot determine the location of his body parts (especially on the left), as he perceives them distortedly and disproportionately. He is unable to copy the pose that is shown to him, because he does not understand how his hands should be positioned in relation to the body (this defect is detected using the Head test. See the figure below). For the same reason, difficulties arise with everyday movements (see Apractoagnosia), which is why everyday skills suffer (the patient loses the ability to dress independently, make the bed, etc.).
Head's test
Unilateral spatial agnosia is also characteristic, when the left half of space, as well as visual, auditory and tactile stimuli on the left, are ignored. When drawing, the patient depicts an object from only one side, usually the right, without drawing the left at all or grossly distorting it.
In addition, with right hemisphere opto-spatial agnosia, the ability to recognize a familiar spatial situation is impaired, as well as to describe the situation from memory.
Right-sided lesions are much more common than left-sided ones.
Diagnostic methods
The Clinical Institute of the Brain has all the conditions for a full diagnosis of patients with agnosia. At the initial stage, it is important to determine exactly what difficulties the patient has with the perception of the environment. For this purpose, there are special tests, during which the patient is asked to describe objects, sounds, and point to parts of the body. After determining the type of disorder, it is important to conduct brain imaging using computed tomography or magnetic resonance imaging. This research method will detect neoplasms, heart attacks, vascular damage and other anomalies that can cause agnosia.
The concept of optical-spatial functions
INTRODUCTION
Relevance of the topic: With normal ontogenesis, by the age of 6 years, that is, in senior preschool age, children have sufficiently formed optical-spatial functions: visual genesis, visual analysis and synthesis, spatial representations, visual-motor coordination, etc.
However, in older preschoolers, as studies by a number of authors show (N.G. Manelis[9], N.Ya. Semago[14], etc.), not only speech disorders are detected, but also deviations in the development of non-speech mental functions, including number and visuospatial functions. This is due to the systemic nature of mental development, the close relationship in the development of speech and non-speech mental processes.
Speech is a way of forming and formulating thoughts and, at the same time, a means of communication, a social connection of influence on others (L.S. Vygotsky). In this regard, it should be emphasized that speech disorders have a negative impact on the formation of non-speech mental functions, including the development of optical-spatial concepts. The presence of children with secondary deviations in the development of mental processes (including optical-spatial representations) creates additional difficulties in the process of speech formation, in mastering knowledge in general, and in developing readiness for schooling.
The lack of development of optical-spatial functions leads to difficulties in differentiating visual images of letters and numbers, to optical dyslexia and dysgraphia, to dyscalculia, which complicates the school adaptation of children and negatively affects the formation of personality.
Thus, the relevance of the problem of studying optical-spatial representations of older preschoolers is due to a number of reasons of a psychological and pedagogical nature; the formation of visual-spatial functions is a significant prerequisite for mastering literacy.
To optimize the process of teaching and raising children of senior preschool age, it is necessary to purposefully study the psychological characteristics of children, identify and determine the qualitative nature of mental development disorders; in this regard, issues related to identifying the psychological mechanisms of disorders associated with the underdevelopment of optical-spatial functions deserve attention.
Purpose of the study: To identify the features of the formation of optical-spatial functions in children of senior preschool age.
To achieve the goal, a number of tasks have been put forward:
1. Analysis of psychological and pedagogical literature devoted to the formation and development of optical-spatial functions in children of senior preschool age.
2. Selection of methods aimed at studying the level of formation of optical-spatial functions in children of senior preschool age
3. Experimental study of the features of optical-spatial functions in children of senior preschool age.
4. Qualitative and quantitative analysis of the obtained experimental data.
Object of study: optical-spatial functions in children of senior preschool age.
Subject of research: features of the formation of optical-spatial functions in children of senior preschool age.
The theoretical significance of the study is that the understanding of the features of optical-spatial functions in children of senior preschool age has been expanded.
Practical significance of the study This study can be used when planning pedagogical work on the upbringing and training of children of senior preschool age.
CHAPTER 1. THEORETICAL ASPECTS OF DEVELOPMENT OF OPTICAL-SPATIAL FUNCTIONS IN SENIOR PRESCHOOL CHILDREN
The concept of optical-spatial functions
Optical-spatial functions are among the most complex mental processes in structure.
Vision is of great importance in a person’s life. This is the main sensory channel that connects him with the outside world. The human visual system is very complex. Thanks to vision, we perceive the world around us in volume and color; we read and watch movies and TV.
In the human visual system, the following levels of signal processing can be distinguished[1]. At the periphery is the retina. During the development of the nervous system, the retina is formed at the earliest stages of development. Therefore, there is every reason to consider the retina “a part of the brain located in the periphery [2].” The next level of processing of visual information is located in the thalamus - this is the lateral geniculate body. Axons of neurons in the lateral geniculate body project to the cortex of the occipital pole of the cerebral hemispheres. The highest stage of visual signal processing occurs in the association fields of the cerebral cortex.
The human oculomotor system performs the following tasks [2]:
1) keeps the image of the external world on the retina motionless while moving relative to this world;
2) identifies certain objects in the external world, places them in the high-resolution retinal area (optic fovea, fovea) and tracks them with movements of the eyes and head;
3) spasmodic (saccadic) movements of the gaze to scan (examine) the external world. Brief information about the structure of the peripheral part of the oculomotor system was given above. Saccades are rapid, friendly deviations of the eyes in the initial phase of the tracking reaction, when the eye jump “captures” a moving visual target, as well as during visual inspection of the external world.
In one case, both eyes move in the same direction relative to the coordinates of the head, in another case, if a person alternately looks at close and distant objects, each of the eyeballs makes approximately symmetrical movements relative to the coordinates of the head. In this case, the angle between the visual axes of both eyes changes: when fixating a distant point, the visual axes are almost parallel, and when fixing a close point, they converge. These movements are called convergent. When looking at objects at different distances, eye movements are convergent and divergent. If the neural system cannot bring the visual axes of both eyes to the same point in space, strabismus occurs[8].
When viewing various objects in the external world, the eyes make fast (saccades) and slow tracking movements. Thanks to slow tracking movements, the image of moving objects is held on the fovea. When viewing a well-structured image, the eyes make saccades alternating with gaze fixation. If a person looks at an image for some time, then the recording of eye movements reproduces quite roughly the contour and the most informative details of the object in question. For example, when looking at a face, the mouth and eyes are especially often captured.
Special experiments have shown that during a saccade, visual perception is blocked [6]. Several mechanisms for this phenomenon can be proposed. It is assumed that during a saccade over a highly structured background, intensity fluctuations at each point exceed the flicker fusion frequency. Another mechanism that blocks visual perception during a saccade is central inhibition. When a moving object appears in the periphery of the visual field, it causes a reflexive saccade, which may be accompanied by head movement. The basis of the neurophysiological mechanism of this reflex is motion detectors in the visual system. Biologically, the reflex is justified by the fact that thanks to it, attention switches to a new object that appears in the field of vision [10].
Higher gnostic visual functions are provided, first of all, by the work of the secondary fields of the visual system (18th and 19th) and the adjacent tertiary fields of the cerebral cortex. Secondary fields 18 and 19 are located on both the outer convexital and inner medial surfaces of the cerebral hemispheres. They are characterized by a well-developed layer III, in which impulses are switched from one area of the cortex to another.
With electrical stimulation of the 18th and 19th fields, not local, point excitation occurs, as with stimulation of the 17th field, but activation of a wide zone, which indicates broad associative connections of these areas of the cortex.
From studies conducted on humans, it is known that with electrical stimulation of the 18th and 19th fields, complex visual images appear. These are no longer isolated flashes of light, but familiar faces, pictures, and sometimes some vague images. Basic information about the role of these areas of the cerebral cortex in visual functions was obtained from the clinic of local brain lesions.
Clinical observations show that damage to these areas of the cortex and the adjacent subcortical zones (“proximal subcortex”) leads to various disorders of visual gnosis. These disorders are called visual agnosia. This term refers to disorders of visual perception that occur when the cortical structures of the posterior parts of the cerebral hemispheres are damaged and occur with the relative preservation of elementary visual functions (visual acuity, visual fields, color perception). In all forms of agnostic visual disorders, elementary sensory visual functions remain relatively intact, that is, patients see quite well, they have normal color perception, and their visual fields are often preserved; in other words, they seem to have all the prerequisites to perceive objects correctly. However, it is the gnostic level of the visual system that is disrupted in them. In some cases, patients, in addition to gnostic ones, have sensory dysfunctions. But these are, as a rule, relatively subtle defects that cannot explain the severity and nature of disorders of higher visual functions.
The main types of optical-spatial disorders are: unilateral spatial agnosia, disturbance of topographic orientation, as well as some manifestations of Balint's syndrome.
The formation of spatial representations begins already in the early stages of ontogenesis; they are basic for the development of many other mental processes [17].
Assessment of the formation of spatial representations and spatio-temporal representations is carried out in the sequence that these levels do not simply “build on top” of each other in the process of development, but intersect in time, overlapping and “embedded” in each other, experience mutual influences and, in general, closely interconnected way. As in the case of studying the voluntary regulation of mental activity, it is necessary to evaluate the “mature”, sufficiently formed level of spatial representations (in accordance with normative or typological concepts) and the closest “deficient” (unformed completely or partially) level or, accordingly, sublevel[8 ].
Treatment of agnosia
Treatment tactics are selected individually. The Clinical Brain Institute employs specialists with extensive experience in treating various types of agnosia. Only some cases require surgery - when tumors, aneurysms, abscesses and other structures are found that need to be removed. In other cases, treatment consists of compensating for lost functions and adapting the patient. For this purpose:
- classes with a speech therapist - special exercises strengthen neural connections and improve perception;
- occupational therapy;
- course of therapy with a neuropsychologist.
Doctors at the Clinical Institute of the Brain insist on full rehabilitation. It can last up to 10 months or more, but qualified medical care will significantly affect the patient’s well-being. Despite the fact that some changes in the structure of the cerebral cortex may be irreversible, it is possible to improve the patient’s quality of life and adapt it in everyday life.
Clinical Brain Institute Rating: 3/5 — 1 votes
Share article on social networks