Modern world neurology has made significant progress in the treatment of multiple sclerosis. If 10 - 15 years ago the prognosis of this chronic disease was often disappointing, and it ended in disability and death, today this scenario can increasingly be avoided.
Our expert in this field:
Lashch Natalia Yurievna
Neurologist of the highest category, candidate of medical sciences, associate professor. Laureate of the Moscow City Prize in the field of medicine.
Call the doctor Reviews about the doctor
This does not mean curing multiple sclerosis completely. But this means preserving a person’s ability to live a full life and avoid loss of ability to work. This means achieving stable, long-term remission, preventing exacerbations or making them rare, minimizing symptoms and residual effects.
Multiple sclerosis has three main forms: relapsing-remitting, secondary progressive and primary progressive.
The relapsing form means the appearance of primary symptoms, which pass relatively quickly, after which remission occurs. In this case, complete recovery occurs, there are no residual effects. This favorable state can last for several years. After this, a relapse occurs, and from now on exacerbations become regular. They occur more frequently and their form becomes more severe. This means that the disease has taken a secondarily progressive form.
After each exacerbation, residual effects persist - muscle weakness, numbness, paralysis, decreased mental performance, deterioration of cognitive abilities and memory.
A person gradually loses the ability to move independently. At first he is forced to rely on a cane when walking, then moves into a wheelchair. This development of the disease is the most typical.
The primary progressive form means the absence of exacerbations and remissions. The disease develops continuously, neurological symptoms increase more and more. Each of the newly appeared symptoms no longer disappears, but remains forever and only gets worse over time.
The latest methods of treating multiple sclerosis that we use give good results in all three forms of the disease. In the relapsing form, they help to prolong remission as much as possible, prevent the onset of a secondary progressive stage, or make it less dangerous. This means avoiding disability.
In the case of a primary progressive form of the disease, our techniques help to slow down the development of the disease and also avoid disability.
Our methods
What are these new techniques that we offer today in our medical center?
First, these are the newest disease- modifying drugs for multiple sclerosis (DMDs). Over the past decades, drugs have appeared that are significantly more effective than anything that was used before. Every year, clinical trials are carried out and new DMTs are introduced into practice. We closely monitor this process and use all the best developments that have proven their advantages.
Secondly, this is a method of preliminary blood purification, which significantly improves the results of drug therapy.
Thirdly, it is a diagnostic method that shows the onset of relapse before symptoms appear. This allows us to take preventive measures and avoid exacerbation or alleviate it as much as possible in order to avoid complications, residual effects and their accumulation, and ultimately disability, and to maintain full physical and mental activity for our patient.
Traditional treatments for multiple sclerosis
Unfortunately, until recently, multiple sclerosis was considered an incurable disease. Traditional methods were aimed at alleviating the symptoms of the disease; they could slow down its development and delay the onset of a new relapse. Drugs - such as interferon, Copaxone or immunosuppressants - suppressed the immune response, inhibited the process of demyelination, but did not restore existing damage to nerve fibers. In other words, they were powerless to restore lost functions to the patient.
Pulse therapy
To relieve acute symptoms of multiple sclerosis, the international clinic Medica24 uses pulse therapy - slow intravenous administration of the hormonal drug - 6-methylprednisolone.
This glucocorticoid drug has a powerful and rapid anti-inflammatory, membrane-stabilizing, anti-edematous effect and helps to significantly improve the patient’s condition within 3 to 7 days.
Before prescribing a course of pulse therapy, our clinic conducts an examination to exclude contraindications.
In particular, gastroduodenoscopy is performed to exclude gastric and duodenal ulcers. Other contraindications must be excluded - infectious diseases, decompensated diabetes mellitus, tuberculosis.
The main advantage of pulse therapy is its exceptional effectiveness. Its results significantly exceed the possibilities of oral use of hormonal or other drugs.
Already in 3 - 7 days, a significant improvement in the condition is achieved - numbness and weakness in the arms and legs disappear, vision improves, dizziness, coordination problems, unsteadiness when walking and other symptoms associated with damage to the spinal cord, cerebellum, and brain stem disappear.
Acute symptoms disappear, the development of the disease slows down, and the condition improves (symptom regression).
The drug 6-methylprednisolone is administered intravenously through a dropper. Treatment protocols correspond to the most effective regimens, the results of which have been objectively confirmed by clinical studies and are today considered the “gold standard” of pulse therapy for multiple sclerosis. In this case, the individual characteristics of the patient are taken into account.
Pulse therapy at the international clinic Medica24 is prescribed based on MRI data with contrast (to identify active foci of demyelination), as well as an assessment of the patient’s condition when new symptoms appear or exacerbation of previous symptoms.
The doctors at our clinic have extensive experience in conducting this type of treatment and timely correction of side effects.
The treatment course is recommended to be carried out in a hospital setting. This guarantees maximum safety and best effectiveness of pulse therapy.
Intravenous administration of a hormonal drug has a powerful therapeutic effect, but along with this there are side effects.
Some of them are relatively minor - dizziness, euphoria, hiccups, nausea, insomnia, anxiety.
Others may be more serious - blood pressure surges, bleeding, hyperglycemia, cardiac arrhythmia.
In order to promptly stop these side effects and adjust the treatment course, it is better for the patient to stay in a hospital, under medical supervision.
We will call you back, leave your phone number
Message sent!
expect a call, we will contact you shortly
Stages of treatment using stem cell transplantation
Step one – Stem cell preparation. First of all, the donor provides doctors with a complete medical history. In addition, tests are taken from the patient, such as blood chemistry, serology for infections, blood type, Rh factor, cardiogram, imaging and spirography are determined. A lumbar puncture and MRI with and without contrast are also required. Hematopoietic stem cells are then extracted from the peripheral blood through subcutaneous injections. This may be enough to transplant stem cells into a patient with multiple sclerosis.
If this method is not effective, then stem cells are collected from the bone marrow of the pelvic bone (iliac crest). This is not a complicated operation, which is performed under local anesthesia, less often - general anesthesia.
Step two – Stem cell transplantation for multiple sclerosis. Before healthy cells are transplanted, a person with multiple sclerosis undergoes a so-called conditioning procedure that suppresses the immune system to prevent it from rejecting the new stem cells. Essentially, this is chemotherapy. Of course, this is a risk, since the immune system is actually destroyed, a person becomes very sensitive to any infections, even a mild cold can be fatal. Therefore, the patient is in a hospital, in a special sterile room. But the period of treatment for multiple sclerosis is short - only a week.
After which, the transplantation itself occurs. Healthy cells are injected into the patient. Then the hardest part is the waiting. The recipient's condition is monitored daily: blood is regularly taken for tests, to check how new stem cells are growing and how the immune system is restored. Most often, it takes 10 to 14 days for test results to return to normal. When this happens, the patient is discharged.
Step three – Treatment of multiple sclerosis and strengthening the immune system. After discharge, the patient must undergo a course of treatment aimed at strengthening the immune system, as well as preventing inflammatory processes. Once every three to four days it is necessary to visit a doctor and take a blood test to monitor the general condition of the patient. The average duration of such treatment is up to two months. After this time and depending on the test results, the doctor sets dates for follow-up studies for multiple sclerosis.
Apply for treatment
By pressing this button, you receive a quick response and an individual decision from the doctor
Diagnostic features
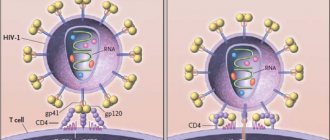
Multiple sclerosis is a disease in which active immune system cells attack and destroy the myelin sheath of nerves. Hereditary factors, intoxication, lifestyle, nervous stress, and acute viral or bacterial infections may play a role in the development of this autoimmune disease. For one reason or another, the immune system begins to behave aggressively towards the body's own cells.
Multiple sclerosis affects the white matter of the brain. Unlike gray matter, which is formed by neurons, it consists of axons. These processes serve as conductors of nerve signals. The shortest of them are only a few millimeters long, the longest - up to one and a half meters or more. Like wires that carry electrical current, axons have an external insulation.
Bundles of nerve fibers, motor and sensory, have the same external insulation. The former are responsible for muscle contractions, the latter for the perception of visual, auditory, olfactory, gustatory, and tactile sensations. The insulating sheath of axons and nerves consists of myelin, a complex protein-lipid substance.
When an autoimmune process develops, aggressive cells of the immune system attack the myelin and destroy it. Areas of exposed axons and nerves arise, in place of which plaques form. Because of this, the speed of transmission of nerve signals decreases sharply (5-10 times). At the same time, the inflammatory process and intoxication develop, which leads to the death of nerve tissue. Because of this, irreversible changes develop, which ultimately lead to disability and death.
The process of formation of compactions and plaques is called sclerosis. These plaques form in large numbers and are scattered throughout the central nervous system - in the brain and spinal cord. Hence the name of the disease - multiple sclerosis.
Slowing of nerve signals and destruction of nerve tissue results in symptoms that usually begin in the legs. An organism affected by a disease can be figuratively compared to a tree whose foliage begins to die and its branches begin to die. While the lower ones have already died, the upper ones look quite healthy. But it's a matter of time. Once the disease has begun to develop, it will spread higher and higher.
First, a person feels weakness and numbness in the feet, then in the legs, and in the hips. Possible sensations of tingling, burning, and crawling. All these are signs of innervation disturbances, which can easily be mistaken for a manifestation of a spinal disease, for example, a protrusion or hernia.
The matter is complicated by the fact that in recent decades degenerative-dystrophic diseases of the spine have become widespread. The doctor prescribes an MRI, which actually shows the presence of a problem, for example, in the lumbar region. This is a very obvious and simple explanation of the symptoms, on the basis of which the doctor prescribes treatment. This may be surgery to remove the disc, which has no effect. Symptoms persist because they are caused by multiple sclerosis. It is good if the disease is diagnosed at least after the first unsuccessful operation.
Weakness in the legs is increasing, but now the genitourinary and excretory systems are involved in the process. The normal processes of defecation and urination are disrupted and occur uncontrollably. Weakness and numbness spread to the hands, it becomes difficult to hold objects, make normal movements, and take care of oneself in everyday life. Moving upward, the disease can lead to paralysis of the respiratory system and heart. The person ends up in the intensive care unit, under a ventilator.
There are times when doctors, having failed to detect multiple sclerosis, instead recommend treating, for example, chronic fatigue syndrome. After all, the central nervous system is not only muscle contractions, but also mental activity. Depending on which nerves are attacked by the immune system, certain initial symptoms of the disease occur. This may be a feeling of constant fatigue, decreased memory, attention, concentration, mental performance, increased fatigue, weakness. Forgetfulness and absent-mindedness appear, which are accompanied by depression or increasing apathy. Sleep becomes intermittent, restless, accompanied by frequent awakenings, nightmares, and insomnia develops. All this can be taken as signs of astheno-neurotic syndrome, or chronic fatigue syndrome. Psychotropic drugs and nootropic drugs are prescribed, which give practically no results. The disease continues to progress.
Early symptoms may also include blurred vision, hearing, poor coordination of movements, and unsteady gait. Such a multiple picture often leads to the fact that a person goes from doctor to doctor, and each one prescribes him a new treatment, conservative or surgical.
Meanwhile, it is enough to do a relatively simple examination to establish the true cause of the symptoms - multiple sclerosis. The basis for diagnosis is MRI data of the brain. Magnetic resonance imaging not only shows foci of demyelination (plaques), but also allows you to distinguish new, young from old. Using a contrast agent, the doctor can see fresh destruction of the myelin sheath of the nerves, as well as areas of inflammation and necrosis of the nerve tissue.
Electroneuromyography is used to assess the speed of transmission of nerve signals. The examination and diagnosis takes only one day.
Another important diagnostic indicator is a blood test for antibodies to myelin. Multiple sclerosis is an autoimmune disease. Based on the content of specific antibodies aggressive to myelin antigens, one can obtain reliable information about the stage of development of the disease and the degree of its danger. The same indicator helps to predict the imminent onset of exacerbation of a secondary progressive form of the disease.
A general immunogram allows you to assess the state of the immune system as a whole and the degree of its changes against the background of multiple sclerosis.
We will call you back, leave your phone number
Message sent!
expect a call, we will contact you shortly
Bone Marrow Transplant Center
What are bone marrow and hematopoietic stem cells? Bone marrow is soft, sponge-like tissue located inside the bone. It contains cells called hematopoietic or blood-forming stem cells. Hematopoietic cells can divide to form more hematopoietic stem cells or develop to create "red blood cells - erythrocytes", "white blood cells - leukocytes" and "platelets". Most hematopoietic stem cells (HSCs) are found in the bone marrow, but small numbers are also found in umbilical cord and peripheral blood. Cells obtained from any of the above-mentioned sources of GCS can be used for transplantation.
What is a bone marrow transplant? Bone marrow transplantation and peripheral blood stem cell transplantation are treatments that use high doses of chemotherapy and/or radiation therapy to suppress damaged HSCs and then replace them with healthy (donor or own) HSCs.
There are three types of transplant: Autotransplantation: Transplantation of the patient's own stem cells. Syngeneic transplant: Transplant by obtaining stem cells from identical twins. Allogeneic transplant: Transplant by obtaining stem cells from siblings or parents. An unrelated donor can also be used if compatible.
How is a bone marrow transplant performed? When transplanting one's own bone marrow cells, radical therapy for the underlying disease is required. Therefore, the patient receives therapy in accordance with the doctor’s prescriptions. Before radical therapy begins, the patient's stem cells are collected and frozen. After stem cell collection, the patient receives high-dose, high-intensity therapy. On average, the duration of such a course of radical therapy is about a week. After completing high-dose therapy, the patient is injected with previously collected healthy stem cells. This method allows you to initiate self-healing of stem cells damaged during therapy.
Are there any risks associated with autologous transplantation? The procedure for collecting stem cells from a patient is associated with the risk of possible introduction of pathological cells into the graft material. In other words, reintroducing a patient's frozen stem cells may cause the disease to relapse due to abnormal cells.
Are there any risks associated with allogeneic transplantation? With an allogeneic transplant, the patient also receives part of the donor's immune system. This is an advantage of the method. However, allogeneic transplantation is associated with the risk of immune system incompatibility. This can cause the donor's immune system to react with the stem cell recipient's organs. There is a risk of damage to the liver, skin, bone marrow and intestines. This is called graft-versus-host disease (GVHD). There are no such risks with autotransplantation.
How are donor stem cells combined with patient stem cells during allogeneic and syngeneic transplantation? Doctors generally use transplanted stem cells that are as similar as possible to the patient's stem cells. In order to minimize potential side effects, the compatibility of the donor and the host is analyzed. On the surface of almost all human cells are protein strands called human leukocyte antigen (HLA antigen). These protein strands are determined using a blood test for HLA antigen typing. In most cases, the success of allogeneic transplantation is based on the degree of compatibility of HLA antigens in the stem cells of the donor and recipient. The chance of donor stem cells being accepted by the recipient's body increases as the number of compatible HLA antigens increases. In general, a high degree of compatibility between the donor's stem cells and the recipient's stem cells minimizes the risk of developing a complication known as graft-versus-host disease (GVHD). Close relatives (especially siblings) are more likely to be HLA-matched than non-relatives. However, only about 25–35% of patients have an HLA-matched sibling. The probability of finding HLA antigen-matched stem cells from an unrelated donor is slightly higher – up to 50%. HLA antigen compatibility among unrelated donors is significantly increased when the donor and host are of the same ethnic and racial background. Although the number of donors is trending upward, some people from certain ethnic and racial groups have difficulty finding a suitable donor. A database of universal voluntary donors can help in finding a compatible unrelated donor. Identical twins have the same genes, hence they have the same HLA antigen strands. In such cases, the patient accepts graft material from his twin. However, the number of such twins is not very large, making syngeneic transplantations a rare occurrence.
How is bone marrow collected for transplantation? Stem cells used for bone marrow transplants are obtained from a liquid core called “marrow.” In general terms, the bone marrow collection procedure, commonly referred to as “harvesting,” differs little for all three types of bone marrow transplants (autologous, allogeneic, syngeneic). During the procedure, the donor receives sedative general anesthesia or local anesthesia, resulting in numbness below the waist. Extraction needles are inserted into the bone marrow of the pelvic bone. Collecting the bone marrow takes about an hour. The collected bone marrow is processed to remove traces of bone and blood. A preservative may be added to the collected bone marrow and then frozen to preserve the stem cells until needed. This method is known as cryopreservation. Using cryopreservation, stem cells can be stored for several years.
How are peripheral blood stem cells obtained? The stem cells used for peripheral blood stem cell transplantation are obtained from donated blood. Peripheral blood stem cells for transplantation are obtained through a procedure called apheresis or leukapheresis. The donor takes special medications for 4 or 5 days before apheresis to increase the number of stem cells in the bloodstream. Blood for apheresis is collected from a large vein in the arm or through a central venous catheter (a flexible tube placed in a large vein in the neck, chest, or pelvis). Apheresis usually takes 4 to 6 hours. The blood is pumped through a machine that collects the stem cells. The blood is then injected back into the donor and the collected stem cells are stored. The stem cells are frozen until they are transplanted into a host.
Are there risks associated with harvesting bone marrow? In general, collecting bone marrow from a donor does not cause problems, since the amount of material extracted is very small. Most of the risks associated with bone marrow harvesting are possible complications related to the use of anesthetics during the procedure. The area where the bone marrow is collected may feel swollen and hard for several days. During this period, the donor may feel tired. The donor's body will replace the lost bone marrow within a few weeks, but the time it takes for the donor to fully recover varies. While some people can return to normal within 2-3 days, some take 3-4 weeks to regain their strength.
Are there any risks associated with donating peripheral blood stem cells? Apheresis usually causes minimal discomfort. The donor may feel weak, trembling, numb lips, and hand cramps. Unlike bone marrow transplant collection, peripheral blood stem cell collection does not require anesthesia. However, drugs used to release stem cells from bone into the bloodstream can cause bone and muscle pain, headaches, fatigue, nausea, vomiting and/or trouble sleeping. Side effects usually subside 2-3 days after taking the last dose of the drug.
What happens after stem cell transplantation into a patient? After entering the bloodstream, the stem cells settle in the bone marrow, where they begin to produce red blood cells, white blood cells and platelets. These cells usually begin to function 2 to 4 weeks after transplantation. Doctors will monitor this with frequent blood tests. Full restoration of the immune system takes a much longer time. This period usually takes several months for patients after autotransplantation and up to 1-2 years for allogeneic and syngeneic transplantations.
What are the potential side effects of a bone marrow transplant? The main risk of both treatments is the patient's increased susceptibility to infection and bleeding due to high-dose/high-intensity therapy. To prevent or treat infections, doctors may prescribe antibiotics to patients. A patient may need a platelet transfusion to prevent bleeding, while red blood cells may be needed to treat anemia. Patients undergoing bone marrow transplant and peripheral blood stem cell transplant may experience short-term side effects such as nausea, vomiting, fatigue, loss of appetite, mouth ulcers, hair loss and skin reactions. Potential long-term side effects are typically associated with pre-transplant chemotherapy and radiation therapy. These include infertility (a person's biological inability to conceive), cataracts (clouding of the lens of the eye), secondary cancer, and damage to the liver, kidneys, lungs and/or heart. The risk of complications and their severity depend on the patient's treatment and these risks should be fully considered and discussed between the doctor and the patient.
What is a “mini-transplant”? A mini transplant is a type of allogeneic transplant (called nonmyeloablative or reduced-intensity transplant). This approach is currently being studied in clinical trials for the treatment of various types of cancer, including leukemia, lymphoma, multiple myeloma and other blood cancers. Mini-transplantation uses low-intensity chemotherapy or low-intensity radiation therapy to prepare the patient for an allogeneic transplant. The use of low doses of anti-cancer drugs and radiation partially destroys the patient's bone marrow, but does not completely destroy it. On the other hand, it reduces the number of abnormal cells and suppresses the immune system to prevent transplant rejection. Unlike traditional bone marrow transplantation or peripheral blood stem cell transplantation, the cells of the donor and the patient continue to coexist for a short period of time after the mini-transplantation. When the bone marrow begins to produce blood, the donor cells enter into a graft-versus-tumor reaction (GVT) and destroy the pathological cells that remain after radical therapy. To enhance the effect of TPE, the patient may be given white blood cells from a donor. This procedure is called “donor lymphocyte infusion.”
Features of treatment
The standard treatment is drugs that correct the functioning of the immune system, reduce its aggressiveness, and suppress pro-inflammatory factors. They are called DMTs—course-modifying drugs for multiple sclerosis. The effectiveness of such treatment may be high or low. They help some, not or hardly help others. In this case, the doctor changes the medications and adjusts the therapy.
The effectiveness of drug treatment depends on two factors. The first is the drugs themselves. Often in our country the same drugs that were prescribed fifty years ago are used. While in world neurological practice much more effective DMTs are used. This is due to the fact that the achievements of world pharmacology are not always properly monitored, and drugs are introduced into practice with a delay. For many patients, this means a poor prognosis for the disease.
We try to avoid this mistake and promptly use all the best, latest, innovative world developments, and use European treatment protocols. The medication course is prescribed and adjusted individually. Neurologists, immunologists, and doctors of other specialties participate in the joint management of the patient. An interdisciplinary approach helps to select the optimal medications and, as a result, achieve stable, long-term remission, eliminate symptoms and allow the person to continue a normal, healthy life.
The second factor is the fundamental feature that distinguishes the treatment of multiple sclerosis in our clinic. Few or almost no one pays attention to it, but in vain.
The fact is that when prescribing certain drugs, doctors almost never attach importance to the most important circumstance - into which blood the active substance enters.
But the blood in multiple sclerosis is extremely polluted. It is saturated with breakdown products of the myelin sheath. It contains a high concentration of antibodies that destroy and have already destroyed myelin. This is a very unfavorable environment, which obviously reduces the effectiveness of the drug or completely reduces it to zero.
But it is enough to remove all these impurities, cleanse the blood, and the effectiveness of the drug increases significantly, sometimes many times over. This makes it possible to obtain completely different treatment results.
You can compare this with a simple example. If the drug is used to treat a runny nose when the nasal passages are blocked and mucus accumulates in them, its effectiveness may be low. But once you clean, thoroughly rinse the nasal passages, and after that apply the treatment, its results will be completely different.
Therefore, before starting a course of drug therapy for DMT, we purify the patient’s blood using plasmapheresis. This procedure consists of separating the blood into red blood cells and plasma, which contains contaminants such as antibodies and myelin breakdown products. After this, the dirty blood plasma is removed and replaced with clean plasma.
After this, the active drug (DITRS) enters the purified blood. The practice of our clinic shows that this sequence of actions allows us to achieve stable remission and restore health even in cases where simple drug therapy has produced virtually no results.
In severe cases, inpatient treatment is required, but outpatient treatment and procedures performed in the day hospital of our clinic are often sufficient to achieve positive results.
results
All 79 patients with a follow-up period of ≥9 months showed clinical improvement or stabilization in the course of the disease. There were no deaths or severe uncontrolled side effects reported during the transplantation. 6 months after transplantation, the distribution of patients according to clinical response was as follows: improvement - 42 (53%) patients, stabilization - 37 (47%) patients. Among the patients with improvement, 20 had a secondary progressive course, 7 had a primary progressive course, 4 had a progressive-recurrent course, and 11 had a relapsing-remitting course. In this group, 25 patients underwent staged transplantation, 15 – early and 2 – salvage transplantation. Of the 37 patients in whom disease stabilization was recorded, 19 had a secondary progressive course, 8 had a primary progressive course, 2 had a progressive-recurrent course, and 8 had a relapsing-remitting course. In this group, 23 patients underwent staged transplantation, 9 – early and 5 – salvage transplantation.
During longer follow-up periods, improvement remained in 40 patients (50.6%), and stabilization in 34 (43.1%). One patient after 6 months and two patients after 18 months of stabilization experienced an increase in the disability index. In two patients, disease progression occurred after 12 and 30 months of clinical improvement. According to MRI, all patients without disease progression after transplantation had no active or new lesions. Overall, 6-year progression-free survival after UDT+AuSCT was 72%. Patients who showed no signs of disease progression did not receive immunomodulatory or immunosuppressive therapy after transplantation. Quality of life monitoring was carried out in 44 patients included in the study. In 40 of them, improvement in quality of life indicators was observed 6 months after transplantation. Improvement in quality of life parameters was established using questionnaires – FACT-BMT and FAMS. 1 year after UDT+AuSCT, the following distribution of patients was recorded in accordance with the degree of response associated with quality of life: 3 patients had a maximum response (more than 75% improvement in the integral indicator of quality of life compared to the baseline); 12 patients had a good response (improvement by 50-75%); 11 patients had a moderate response (25-50%); in 13 there was a minimal response (improvement of less than 25%) and in 5 patients there was no response related to quality of life. It should be noted that patients with a longer follow-up period showed further improvement in quality of life indicators. The article presents a classification of types of transplantation for multiple sclerosis, based on the concept of VDT + HSCT for autoimmune diseases.
Condition monitoring
Another feature of our approach to treating multiple sclerosis is control of the condition. Regular tests make it possible to anticipate and prevent exacerbation of the disease in time, to catch it at a stage when it has not yet had time to lead to irreversible consequences.
This means that a person continues to live a healthy, normal, fulfilling life, monitoring his condition from time to time. To do this, it is enough to do a blood test once every three months for the presence of antibodies to myelin.
It would seem that everything is simple. But it is surprising that such an effective method is practiced relatively rarely; treatment usually begins after the symptoms of an exacerbation appear. But it can be avoided. It never arises suddenly and instantly. It is preceded by an increase in specific antibodies in the blood. Regular monitoring of these indicators is enough to completely control a person’s condition.
In practice, this means that a person has completed a course of drug therapy, as a result of which remission was achieved. The symptoms have disappeared and the person continues to live a normal life. From time to time he comes to our center and does a blood test for antibodies.
They can remain at low levels for a long time. This means that there is no threat to health. But suddenly another analysis shows a significant increase in the level of antibodies. This means that if measures are not taken, an exacerbation will soon occur.
Forewarned is forearmed. We take preventive measures and aggravation is avoided. This may be plasmapheresis or its combination with drug therapy, it all depends on the individual case.
We will call you back, leave your phone number
Message sent!
expect a call, we will contact you shortly
Diagnosis of multiple sclerosis
The neurologist conducts a thorough examination, collects data on the time of onset of the first symptoms, and checks reflexes. To make an accurate diagnosis and subsequent treatment of multiple sclerosis, a CT scan, MRI of the brain and spinal cord, and an immunogram are needed.
The diagnosis of “multiple sclerosis” in our time has ceased to be synonymous with the word “hopelessness”! Effective and safe treatment exists!
To get advice on the treatment of multiple sclerosis in Moscow, call us by phone and fill out a request for a call back