Attention!
The information in the article is for reference only and cannot be used for self-diagnosis or self-medication. To decipher the test results, contact a specialist.
Previously, this condition was considered normal age-related changes that accompany the aging of the body. Now they are trying to identify it in patients as early as possible in order to slow down the process of neuron degradation with the help of drugs.
Alzheimer's disease - what is it?
Alzheimer's disease is a progressive form of senile dementia that leads to the loss of cognitive abilities. It belongs to the group of acquired neurodegenerative pathologies. The disease occurs more often in patients over 65 years of age. Forms that begin before 60 years of age are less commonly noted. The disease develops gradually and unnoticed.
The patient first develops short-term memory and attention disorders. Then the symptoms increase steadily. A person's attention, memory, and speech are severely impaired. The patient cannot develop new skills and reproduce old ones. His psychomotor coordination is impaired and his time orientation suffers.
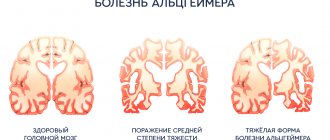
The patient is disoriented in space, place and self. Identifies thought disorder. All pathological processes are caused by the destruction of brain cells. There are two types of Alzheimer's disease. The first is an early onset of the disease with the onset of clinical manifestations after 65 years, the second type with the onset of symptoms before 65 years.
The diagnosis is made based on the clinical picture after excluding diseases with a similar clinical picture. The diagnosis is confirmed posthumously during an autopsy. The number of neurofibrillary tangles and senile plaques is determined.
The role of diet in the development of Alzheimer's disease
15.12.2020 1859
Regular consumption of certain foods, including cheese and red wine, may slow cognitive decline and prevent the development of neurodegenerative diseases such as Alzheimer's disease. This conclusion was reached on the basis of a large-scale study by scientists from the University of Iowa (USA). The researchers' results were published in the latest issue of the American medical journal Journal of Alzheimer's Disease.
The diet, the food that a person consumes throughout life and especially in old age, affects not only his behavior in general, but also significantly affects his cognitive abilities, the study notes. “Our work is essentially the first to address the relationship between diet and cognitive processes, especially in old age,” says project leader and assistant professor at Iowa State University Auriel Willette. According to him, an extensive database provided by the British Biobank, which contains a variety of information on more than half a million patients, including genetic data, clinical test results, helped track the lifestyle and health status of 1,787 people aged 46 to 77 years. functional studies. In order to identify the degree of preservation of cognitive functions, respondents were offered a test - Fluid Intelligence Test (FIT). The baseline level of cognitive ability was compiled based on the results of surveys during 2006–2010, the next phases of research were distributed between 2013–2015 and 2015–2016. In addition, patients answered questions about their food preferences and alcohol consumption, especially wine, beer and spirits. The results of the study showed that cheese and red wine are precisely the foods whose consumption protects the human brain from cognitive “failures” even at a later age. According to scientists, weekly consumption of lamb also helps maintain the cognitive functions of older people at the proper level. Researchers have not fully clarified the role of excess salt in the diet, but they still recommended that people with a predisposition to neurodegenerative diseases limit their intake. “Our work clearly demonstrates the role of cheese and red wine in preventing intellectual loss in the elderly,” says Willet. — In the midst of the coronavirus pandemic, this diet allows you to maintain your body in good shape even at a late age. This is very important as we all know how difficult it can be to manage dementia care under conditions of self-isolation and distancing.” Co-author of the study, Ph.D., Iowa State University neurologist Brandon Klinedinst, is convinced that “nutrition correction is one of the mechanisms for regulating the human information system at the genetic level, which can help a person maintain intelligence at any age.” Source: TASS News Agency https://content.iospress.com/search?q=Klinedinst&published_between=&from_year=&to_year=
Share the news on social networks
Previous news Next news
16.12.2020
The cause of schizophrenia may be a defect in the human immune system...
1139
13.12.2020
The law on reform of the compulsory medical insurance system has been published
1675
All news
Stages
The course of the disease is divided into four phases, with a progressive clinical picture with cognitive and functional impairment. The following stages are distinguished:
- Predementia. The first manifestations of Alzheimer's disease are often similar to a reaction to stress or normal age-related changes. Changes in cognitive function are detected eight years before the advanced stage during neurocognitive testing. Problems begin with the inability to assimilate new information. Patients cannot concentrate. Planning suffers and cognitive flexibility is lacking. Abstract thinking is impaired, semantic memory is reduced.
- Early dementia. Progressive memory deterioration and impairment of all types of perception in Alzheimer's disease lead to confirmation of the diagnosis. Memory declines unevenly. Old memories of your life and long-learned facts are preserved. Recently learned facts are quickly forgotten. Speech disturbances appear. Defects in executive functions, motor disorders, and perception disorders occur. Vocabulary depletion occurs and speech fluency decreases. Clumsiness appears when using fine motor skills, and problems with coordination increase. The person is able to perform only simple tasks independently.
- Moderate dementia. Patients experience progressive deterioration of their condition. The possibility of independent action is reduced. Speech disorders become obvious, and the vocabulary is sharply depleted. The person misunderstands the meaning of the word. Reading and writing skills are lost. Coordination is impaired during complex sequential movements. The person cannot cope with most ordinary tasks. The patient does not recognize close relatives. Long-term memory deteriorates. Neuropsychiatric changes appear - irritability, wandering, emotional lability, spontaneous aggression.
- Severe dementia. At this stage of the disease, the patient is dependent on outside help. He uses single phrases and words when communicating. Then speech disappears completely. The reaction to emotional appeals to them remains. Sometimes episodes of aggression occur, which are replaced by apathy and exhaustion. Even the simplest actions are impossible without outside help. The patient's muscle mass decreases. He moves with difficulty, often unable to get out of bed.
Death occurs from associated causes - pressure ulcers, pneumonia and other diseases.
How to organize effective nutrition for Alzheimer's disease?
Patients with neurological diseases and their loved ones are subjected to a range of tests. Most of them are related to nutrition. Neurological diagnoses are most often accompanied by problems with chewing, swallowing and digesting food. Because of this, patients cannot eat properly, lose weight, their body is depleted and becomes susceptible to various infections. As a result of brain damage, patients often have difficulty coordinating movements and caring for themselves, which also makes it difficult to prepare and eat food. Chronic insufficiency of blood supply to the brain and death of neurons lead to the development of dementia in the patient. In these cases, doctors often advise considering nutritional support. Enteral nutrition helps fight or prevent malnutrition, facilitates the process of eating and simplifies the care of a sick person. Timely selection of nutrition will make it possible to correct the symptoms of the disease and improve the general condition of the patient. The doctor will help you choose the right therapeutic food and calculate its amount in accordance with your individual energy and protein needs, taking into account your diagnosis, age and general condition of the body.
Dietary problems in patients with Alzheimer's disease:
- Risk of weight loss. People with Alzheimer's disease suffer from memory impairment: they may forget to eat, fail to notice that they are hungry, or fail to recognize food at all. Also, due to little physical activity, they may lack appetite, and medications can change their sense of smell and taste. Because of this, patients eat little, sometimes refuse food altogether, and as a result they can lose a lot of weight, their body can be so weakened that the risk of falls, injuries and various diseases increases. In these cases, protein-rich foods and sufficient fluids are recommended.
- Large appetite, lack of feeling of satiety. Some patients with Alzheimer's disease, on the contrary, eat a lot of sweets. In this case, it is important to monitor the patient and try to keep the diet varied and nutritious. But this should be done carefully: sudden menu changes and restrictions can cause stress in the patient.
- Difficulties with self-care. At certain stages of Alzheimer's disease, patients find it difficult to eat on their own: it is difficult to hold a spoon or put the required amount of food on a plate, etc. In this case, you need to gently remind the patient about the need to eat; it is better to arrange meals together. It is important to prepare food and drinks at the required temperature and consistency in advance.
- Constipation, nausea, bloating. This problem is very common among patients with Alzheimer's disease. In this case, increasing physical activity, including foods rich in fiber, and drinking plenty of fluids can help.
Recommendations for organizing nutrition for patients with Alzheimer's disease:
- The patient should be reminded of the need to eat.
- It is better to sit at the table in a quiet environment so that the patient is not distracted by extraneous noises (TV, radio, etc.)
- There is no need to rush the patient; on the contrary, you should ask him not to rush and calm him down if something doesn’t work out.
- The patient should be in a normal mood, he should not be excited or depressed. Don't force feed him.
- Drinks and food should be at normal temperature. They should be cooled or heated in advance: the patient may lose the feeling of cold and hot.
- It is better to serve food that can be eaten with your hands, because... At certain stages of dementia, the patient may not be able to use cutlery or may injure himself.
- In the later stages of dementia, food should be liquid or pureed.
- Say the names of the dishes and drinks you serve. This way the patient will be able to retain them in memory longer, and this will make your communication easier.
- It is important to monitor the diet: the patient must receive the right amount of nutrients.
Instead of a conclusion:
Nutrition directly affects the development of Alzheimer's disease. A healthy diet for older adults can improve cognitive function, slow progression, and alleviate dementia. Once a diagnosis has been made, a nutritional support plan should be developed with the attending physician to ensure that the patient receives the required amount of nutrients and maintains a good standard of living. Share:
(3 ratings; article rating 2.7)
Causes
A single factor responsible for the occurrence of Alzheimer's disease has not been identified. It is believed that there is a hereditary predisposition to the disease. Several hypotheses for the formation of changes in the brain are now being put forward:
- Cholinergic. Cognitive deficits are associated with decreased production of the neurotransmitter acetylcholine. The theory is considered outdated, but it is not completely abandoned.
- Amyloid. The main factor in the development of changes in the brain in Alzheimer's disease is considered to be the deposition of beta-amyloid protein in its tissues. A mitochondrial DNA defect is found in half of the patients. The gene encoding its formation is located on chromosome 21. The early onset of the disease is associated with defects in the PSEN1, APP, and PSEN2 genes. Beta-amyloid plaques appear in the brain, slowing down the speed of cognitive reactions. This hypothesis is recognized as the main one. Amyloid accumulation sets off a chain of neurodegenerative disorders.
- Tau hypothesis. It is believed that a cascade of pathological changes initiates a deviation in the structure of the tau protein. In it, hyperphosphorylated threads are connected. Neurofibrillary tangles are formed in neurons. Then the disintegration of microtubules occurs. The transport system in cells is destroyed. This disrupts the signal transmission system between neurons.
- Infectious. It is believed that the development of the disease is associated with the causative agent of periodontitis. Colonization of brain tissue by bacteria occurs, which increases the production of beta-amyloid.
Researchers note that high sugar consumption accelerates the development of cognitive impairment. This worsens the course of the disease.
PsyAndNeuro.ru
Currently, WHO recommends prescribing cholinesterase inhibitors for the treatment of Alzheimer's disease for mild to moderate dementia, and memantine for moderate and severe dementia. Also, aducanumab was approved this year, but its place in the treatment of pathology has not yet been fully determined.
The results of clinical trials, which inform decisions about the development of new drugs, are usually presented as comparisons of quantitative differences between groups on relevant symptom scales. To interpret clinical trial results, make clinical decisions, and design studies with sufficient statistical power, it is necessary to decide what treatment effect qualifies as a minimum clinically important difference (MCID). In Alzheimer's disease (AD) research, there is no consensus on MCID. Although the US Food and Drug Administration (FDA) issued guidelines for the approval of new antidementia drugs in 1989, there is still no precise definition of MCID.
The FDA's Peripheral and Central Nervous System Advisory Committee voted almost unanimously on November 6, 2021, against the approval of aducanumab. However, his recommendation was rejected and the FDA eventually approved the drug for the treatment of AD. The situation with aducanumab forces us to revisit the question: how to determine the effectiveness of antidementia treatment?
In 1989, the same FDA Advisory Committee decided that a difference of 3 points on the ADAS-Cog asthma symptom rating scale was an indication of a clinically significant change in the patient's condition. However, the presence of a statistically significant difference may be due to chance. Any effect larger than the null effect may be statistically significant if the sample size is large enough. Thus, there is still no consensus on the issue of MCID in AD treatment trials.
The FDA recognizes treatment for mild to moderate AD dementia as effective if there is a positive change in the main symptoms (cognitive function) and global clinical picture (as assessed by the attending physician) or in functionality (the patient's activity in daily life). For studies involving prodromal patients with mild cognitive impairment, the FDA requires evidence of only statistically significant changes in prespecified measures that include cognitive and daily functioning. In 2013, the FDA recommended the use of a comprehensive assessment tool, the Clinical Dementia Rating Sum of Boxes (CDR-SB). A statistically significant improvement in CDR-SB is shown when changes in basic symptoms (memory, orientation, problem solving, logical thinking) are recorded and functionality (everyday life, daily activities, hobbies) improves at the same time. The European Medicines Agency has a similar approach. However, the question remains - is the bar set too low for determining effectiveness?
A 2021 study found that MCID increases with disease severity. For mild cognitive impairment and mild AD, the MCID is 0.98 and 1.63 points on the CDR-SB scale, and 1.26 and 2.32 points on the MMSE scale, respectively. A 2012 study reported that the MCID in patients with mild AD was 3 on the ADAS-Cog11 scale.
However, these MCID values are not a requirement for FDA approval. Notably, neither the CDR-SB nor the MMSE MCID thresholds were met in the aducanumab trials (CDR-SB -0.39; MMSE 0.6).
Memantine and other approved antidementia drugs are safe and well tolerated, while high doses of aducanumab are associated with a 35% chance of cerebral edema, a 20% chance of microbleeds in the brain (in the placebo group, 2% and 7%, respectively). Side effects increase the risk that blinding in the high-dose aducanumab arm will be compromised and will therefore confound the outcome of caregiver-administered questionnaires.
The small effect of aducanumab is comparable to that shown by other drugs that target amyloid. It is likely that amyloid reduction in itself does not lead to a clinically significant improvement in cognitive function, while the use of memantine has a significantly positive effect on these indicators. A 2021 meta-analysis showed that a 0.1 SLA unit reduction in amyloid levels with aducanumab resulted in a 0.03 point improvement in MMSE, while Memantal* showed an increase in amyloid levels over 3 months of therapy. indicator by 2 points.
Regulators' low bar for assessing effectiveness encourages study sponsors to increase sample sizes in order to be more likely to find a statistically significant change. For example, a 78-week trial of aducanumab was planned to include 1,350 participants, but the number was increased to 1,647 when it became clear that a statistically significant change might not be detected.
Clinical studies of cognitive impairment should be designed to ensure that their results reflect meaningful changes. Guidelines for trials of new AD drugs should include definitions of clinically significant changes in at least the CDR-SB and MMSE scores. The use of a clearly defined MCID will provide clarity and confidence in trial results, which will provide significant benefits to patients and the healthcare system as a whole.
*Memantal is memantine produced in the EU by Sinton, Spain. Delivered to Russia, Great Britain, Holland, France, Germany and other countries.
Author: Filippov D.S.
Source: Liu K., Schneider L., Howard R. The need to show minimum clinically important differences in Alzheimer's disease trials // Lancet Psychiatry, Published Online June 1, 2021
Symptoms
The initial signs of change are almost noticeable. Manifestations of the disease develop gradually and slowly, they are as follows:
- the patient has difficulty remembering recent events;
- there are emotional disorders;
- poor recognition of famous objects;
- higher cortical functions are disrupted;
- decreased ability to navigate in space;
- depression;
- indifference;
- anxiety.
Subsequently, the patient's cognitive impairment increases. He is incapable of making decisions. Mathematical operations are difficult to complete, making it difficult to count money. Speech becomes incoherent. Long pauses appear, which are associated with a long selection of words. The late stage of the disease is characterized by the following clinical picture:
- rave;
- failure to recognize loved ones;
- hallucinations;
- convulsions;
- shuffling gait;
- loss of ability to move independently;
- personality degradation;
- disturbance of orientation in place and time;
- lack of opportunities for mental activity.
In severe dementia, the patient is completely dependent on others. He can't serve himself. Acquired skills disappear, articulate speech is lost. Aggression alternates with apathy and exhaustion.
Diagnostics
If a disease is suspected, patients consult a psychotherapist or neurologist. The doctor examines the patient and studies his medical history. Talks with the patient and his relatives. The main criterion for diagnosis is the presence of decreased memory and cognitive abilities. Additional research methods are prescribed:
- CT and MRI of the brain;
- cerebrospinal fluid analysis for beta-amyloid protein;
- NuroPro test;
- genetic testing;
- determining the level of amyloid beta in the blood;
- positron emission tomography.
The patient is given tests to determine cognitive abilities - digital, Sage test, watch image.
Treatment
To date, no treatment has been found to stop the development of Alzheimer's disease. There are medications that slow the progression of symptoms. These include the following drugs:
- NMDA antagonists;
- cholinesterase inhibitors;
- beta-secretase inhibitor.
To relieve symptoms, antipsychotics and drugs that increase cerebral circulation are prescribed. A low-calorie diet enriched with protein is prescribed. It is recommended to reduce the amount of sugar and salt. You need to eat fatty fish, foods high in B vitamins, selenium, and zinc.
Psychotherapeutic support plays an important role in improving the patient’s well-being. It is important for the patient to avoid stressful situations and stay in comfortable conditions. He needs to create a positive emotional mood.
Second-line drugs for the treatment of Alzheimer's disease
The most effective drugs for Alzheimer's disease are cholinesterase inhibitors. However, treatment of the pathology should be comprehensive with the elimination of clinical manifestations.
What medications treat Alzheimer's disease:
- Glycine can be used to improve cerebral circulation and normalize the emotional background;
- To eliminate hallucinations and the appearance of obsessions, antipsychotics and tranquilizers can be used;
- Treatment of anxiety, panic attacks, and depression is carried out with the help of antidepressants.
All drugs for the treatment of Alzheimer's disease must be prescribed by the attending neurologist. Each of the drugs has its own contraindications and side effects, so using them independently can negatively affect your health.
In addition to drug treatment, the patient is prescribed other types of therapy:
- Physiotherapy;
- Aqua aerobics;
- Art therapy;
- Special classes to improve cognitive functions.